

Learn more about intermittent catheters
The rigidity of intermittent catheters vary. The softer versions often come with an outer insertion sleeve or a gripper. The function of the sleeve and the gripper is to enable the user to grab the catheter at any point upon the insertion. Both sleeve and gripper are useful to control a catheter that is made of a soft material, as it might bend outside the urethra when inserted. Firmer catheters can be inserted in a smoother movement, as they can overcome normal resistance in the urethra.
Intermittent catheterisation methods
- Clean: The clean technique is defined by self-catheterisation with a no-touch technique. This means that the person doing the catheterisation has direct contact with the catheter connector, but the catheter itself must not be touched. When using clean technique there is a potential risk of contamination, and it is important to wash both hands as well as the opening to the urethra thoroughly with soap and water. Always follow the instructions provided by the manufacturer. The clean technique is used outside of hospitals (1).
- Sterile: The sterile technique is defined by a catheterisation where the person inserting the catheter is wearing sterile gloves and has no direct contact with the catheter. The technique is often performed by health care professionals in hospital settings (1).
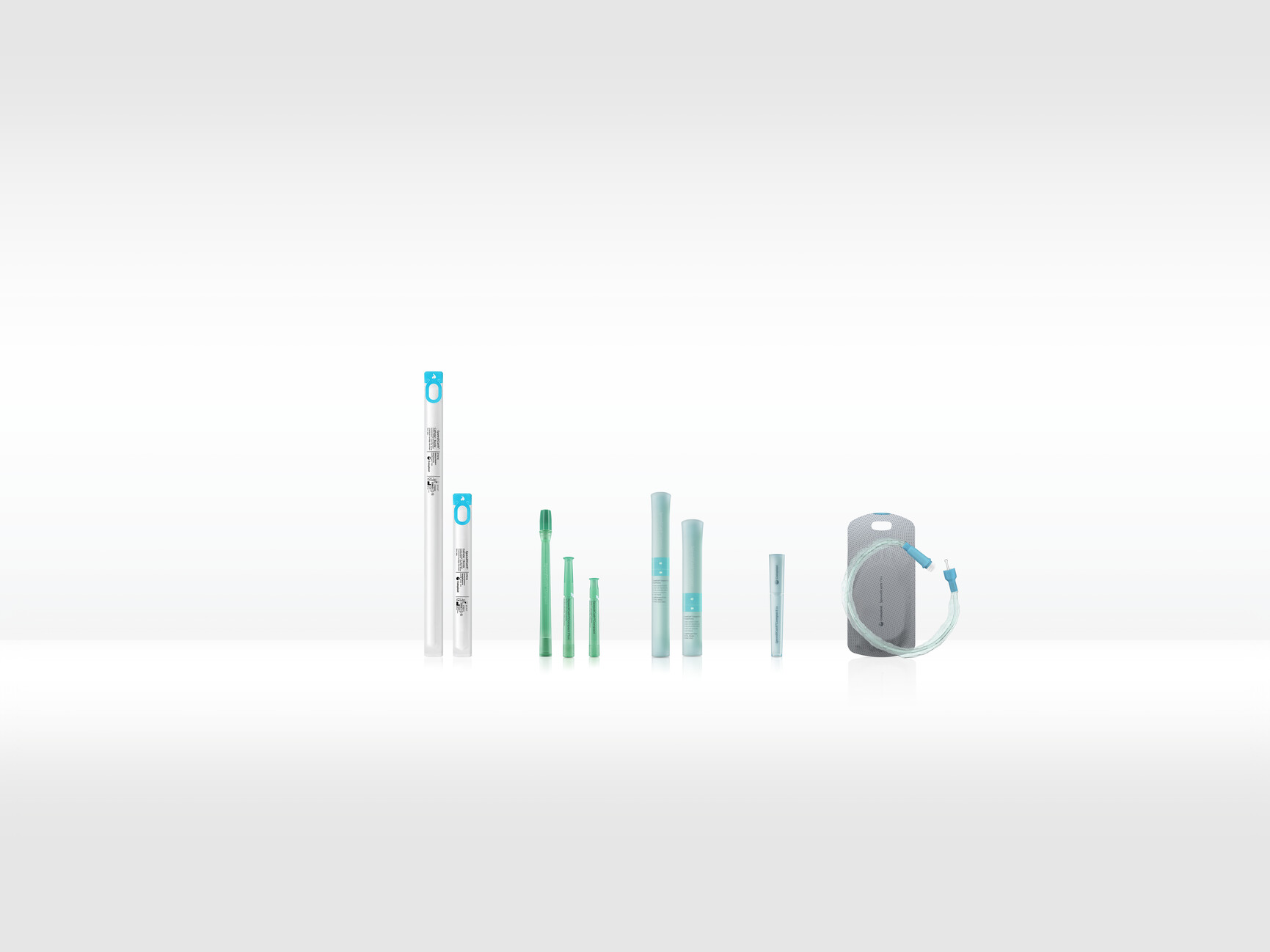
Catheter types
- Standard catheters: Standard catheters are the most common catheter type. These catheters are primarily straight and typically come in standard lengths of approx. 40 cm for men and approx. 20 cm for women. The firmness of standard catheters varies.
- Compact catheters: Most compact catheters are similar to the standard catheters, but shorter and packed more discrete. Often, they are easier to use due to the shorter length (kilde).
- Sleeve catheters: The sleeve catheters are soft catheters covered with an insertion sleeve. The sleeve protects the catheter from contamination during insertion.
- Catheter sets: Catheter sets are standard, compact or sleeve catheters pre-connected with a drainage bag to collect the urine.
Catheter tips
- Nelaton tip: Is defined by a straight tip and is for both men, women, and children with no special catheter needs
- Tieman/coudé tip: Is defined by a curved tip and is primarily for men. The tips design to make it easier for men with enlarged prostate to insert a catheter.
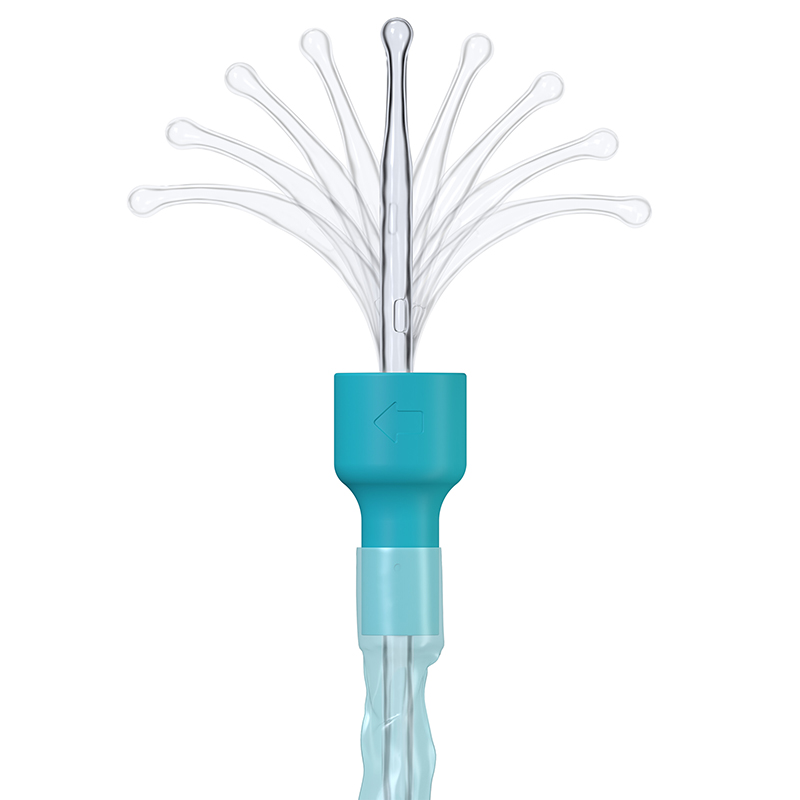
- Flexible tip: Is defined by a flexible often ball shaped tip which gently guides the catheter through any curves or bends in the urethra.
Catheter eyelets
Most intermittent catheters come with two eyelets or holes close to the catheter tip. The urine is drained when the eyelets reach the bladder.
The shape, size, positioning, manufacturing process and surface treatment of the eyelets are important for how the catheter performs and how gentle it is to the urethra.
Coating on intermittent catheters
To insert an intermittent catheter in the most safe and comfortable way, it needs to be lubricated. A slippery surface eases the insertion and reduces the risk of damaging the urethra. There are several kinds of surface treatments for intermittent catheters.
- Uncoated: Catheters which must have a gel added manually before use.
- Gel coated: Catheters that are coated in gel and can be inserted without any further preparation. The challenge with gel coated catheters is that the coating can be rubbed off during insertion leaving the catheter uncoated. The coating can be left in the urethra and bladder when removing the catheter.
- Hydrophilic coated: Catheters that are pre-coated with a dry hydrophilic coating. The coating needs to be activated by adding drinking or sterile water for 30 seconds. This will allow the coating to swell into a slippery smooth layer. The coating layer stays on the surface of the catheter during use.
- Hydrophilic coated ready to use: Catheters that are coated with a hydrophilic coating and come immersed in water, ready to use so you don’t need to bring nor think about access to water no wait for optimum hydration of the coating (13,14).
|
|
Uncoated |
Gel coated |
Hydrophilic coated |
Hydrophilic coated ready to use |
|
Ready to use |
No – gel needed |
Yes |
No – water needed |
Yes |
|
Homogenous surface when inserting |
No – gel can move around and smear |
No – gel can move around and smear |
Yes, if hydrated correctly |
Yes |
Catheter sizes
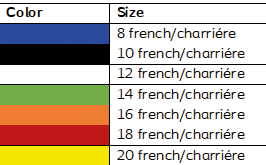
It is key to the success of the catherisation to find the right catheter size. The size of an intermittent catheter refers to the outside diameter of the catheter. The measuring unit is used in 1/3 mm and is referred to Charriére or French. The size should not be too big as this might complicate insertion. The size should not be too small as the urine might then flow on the outside of the catheter. In general, the bigger size, the better flow. However, several specific parameters such as the inner diameter (ID), the tip inlet area to inner lumen area ratio (AR), and resistance from the inlet tip also influence catheter flow rates. Hence, it is not possible to predict the actual flow rate of urinary catheters based on the packaging information or specifications (Ref: Journal of Pediatric Urology (2017) 13, 377.e1e377.e6).
Often the size of the catheter can be identified by the color of the connector.
Literature
- Balhi S, Mrabet MK. Teaching patients clean intermittent self-catheterisation: key points. Br J Community Nurs. 2020 Dec 2;25(12):586–93.
- Weld KJ, Dmochowski RR. Effect of Bladder Management in Urological Complications in Spinal Cord Injured Patients. J Urol. 2000 Mar;163(3):768–72.
- Krebs J, Wöllner J, Pannek J. Risk Factors for Symptomatic Urinary Tract Infections in Individuals with Chronic Neurogenic Lower Urinary Tract Dysfunction. Spinal Cord. 2016 Sep;54(9):682–6.
- Esclarín De Ruz A, García Leoni E, Herruzo Cabrera R. Epidemiology and Risk Factors for Urinary Tract Infection in Patients with Spinal Cord Injury. J Urol. 2000 Oct;164(4):1285–9.
- Wyndaele JJ, De Sy WA, Claessens H. Evaluation of Different Methods of Bladder Drainage Used in the Early Care of Spinal Cord Injury Patients. Spinal Cord. 1985 Feb;23(1):18–26.
- McGuire EJ, Savastano J. Comparative Urological Outcome in Women with Spinal Cord Injury. J Urol. 1986 Apr;135(4):730–1.
- Vahr S, Cobussen-Boekhorst H, Eikenboom J, Geng V, Holroyd S, Lester M, et al. Catheterisation: Dilatation, Urethal intermittent in adults. EAUN, European Association of Urology Nurses; 2013.
- Jeffery N, Mundy A. Innovations in indwelling urethral catheterisation: Indwelling urethral catheterisation innovations. BJU Int. 2020 May;125(5):664–8.
- Hunter KF, Bharmal A, Moore KN. Long-term bladder drainage: Suprapubic catheter versus other methods: A scoping review. Neurourol Urodyn. 2013 Sep;32(7):944–51.
- Faure A, Cooksey R, Bouty A, Woodward A, Hutson J, O’Brien M, et al. Bladder continent catheterizable conduit (the Mitrofanoff procedure): Long-term issues that should not be underestimated. J Pediatr Surg. 2017 Mar;52(3):469–72.
- Schurch B, Tawadros C, Carda S. Dysfunction of lower urinary tract in patients with spinal cord injury. In: Handbook of Clinical Neurology [Internet]. Elsevier; 2015 [cited 2021 Oct 12]. p. 247–67. Available from: https://linkinghub.elsevier.com/retrieve/pii/B9780444632470000146
- James RE, Palleschi JR. Suprapubic Tap or Aspiration. In: Pfenninger and Fowler’s Procedures for Primary Care. Elsevier; 2011. p. 784–5.
- Andersen MJ, Flores-Mireles AL. Urinary Catheter Coating Modifications: The Race against Catheter-Associated Infections. Coatings. 2019 Dec 29;10(1):23.
- Dellimore KH, Helyer AR, Franklin SE. A scoping review of important urinary catheter induced complications. J Mater Sci Mater Med. 2013 Aug;24(8):1825–35.