
The Wound Care Pathway: Your 5 step guide to wound healing
PDF
6MB
25
pages
By following the steps in this pathway, you can provide an optimal healing environment for burns and reduce the risk of complications that could lead to delayed healing or worse.
Any advice included here needs to work in conjunction with your local protocols and your individual scope of practice.
This article is based on the book A pathway for treating a person with a: Burn
Burns are injuries to the skin that occur when the skin or other tissues are damaged by contact with heat (flame, scalds from liquids spilled or liquid immersion, grease or steam), electricity, radiation or chemicals. Burn injuries can be devastating and without appropriate treatment can result in slow healing, infection, scar formation, disfigurement, contractures, joint dysfunction, pain, and psychological and spiritual stress.1
The severity of a burn relates to both the depth of skin involvement and the percentage of the total body surface area involved.2
This pathway is focused exclusively on thermal burns, including scalds, in patients of all ages.

A thermal burn

A scold
For more information, consult The Wounds Canada best practice recommendations for the prevention and management of burns and/or The Wounds International Best Practice Guidelines.
The guidance provided in this Wound Type Specific Pathway, is best understood in combination with the detailed guidance available to you in The Wound Care Pathway.
➔ Ensure the safety of the patient and carer/clinician by removing patient from source of injury.
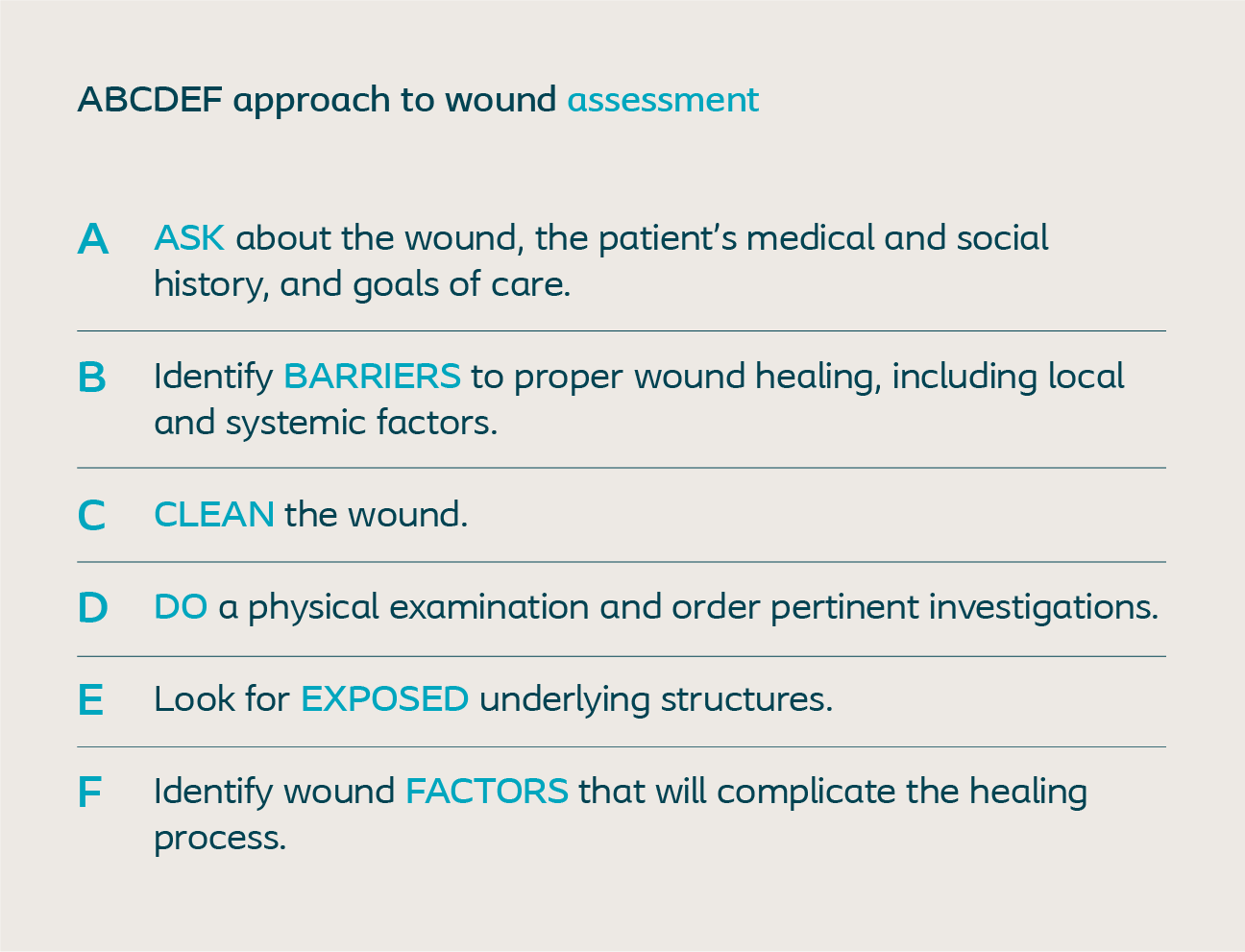
➔ Immediately conduct a primary ABCDEF assessment (see below).
➔ Next, stop the burning process by flushing with body temperature running water or by using water-soaked towels for 20 minutes. Do not use cold water, ice or frozen materials
Cool the burn not the patient.
➔ Conduct a burn assessment to determine the Total Body Surface Area of the burn (TBSA), as well as the mechanism, location, depth and size.

Superficial partial thickness burn

Deep partial thickness burn
The patient’s palm area (palm and digits) approximates to 1% of the total body surface area.
➔ Document the cause of the burn, when the burn occured and what has been done so far.
➔ Location of the burn:
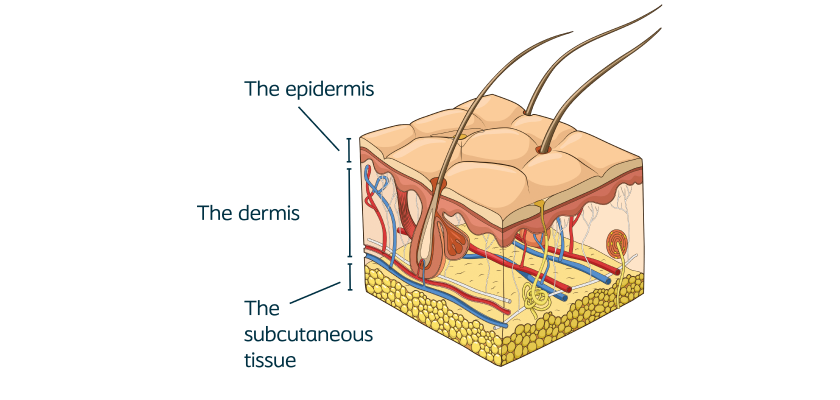
➔ Measure the depth of the burn:
-Superficial – only the epidermis is damaged – often associated with sun burns with no blisters.
-Superficial partial thickness – extends to upper layers of the dermis, is painful and blisters are present.

A blister requiring deroofing

Superficial partial thickness

Deep partial thickness

Full thickness burn

Severe full thickness
Layers of skin affected:
The epidermis is affected, but the dermis is intact.
Skin examination:
The skin is red and painful, but not blistered. Capillary refill* blanches then rapidly refills.
Layers of skin affected:
The epidermis and upper layers of dermis are involved
Skin examination:
The skin is red or pale pink and painful with blistering. Capillary refill* blanches but regains its colour slowly.
Layers of skin affected:
The epidermis and the upper and deeper layers of the dermis are involved, but not underlying subcutaneous tissues.
Skin examination:
The skin appears dry, blotchy or mottled, red, and typically painful (due to exposed superficial nerves). There may be blisters. Capillary refill* does not blanch.
Layers of skin affected:
The burn extends through all the layers of skin to subcutaneous tissues. If severe, it extends into muscle and bone.
Skin examination:
The skin is white, brown, or black (charred) in colour, with no blisters. It may appear dry, leathery, or waxy and is painless. Capillary refill* does not blanch.
➔ Conduct a wound assessment using a validated wound assessment tool.
➔ Conduct a holistic patient assessment to determine comorbidities, allergies, etc.
➔ Check for tetanus vaccine status.
➔ Conduct a pain assessment.
➔ Conduct a complete physical exam to check for other injuries, including inhalation injuries.
➔ It is important to remove jewellery or clothing which may have a tourniquet effect if edema becomes an issue or can be a source of thermal insulation preventing the burn from cooling.
➔ Also evaluate the burn pattern for consistency with the history of injury to evaluate for Non-Accidental Trauma. If this is suspected, it should be reported in accordance with local laws and regulations.
Complications with even small burns in children can be fatal (toxic shock syndrome) and should be referred.6
➔ A treatment or care plan should be developed in partnership with all members of the care team and the patient.
➔ When developing a treatment plan consider the following:
-Eat a high-calorie/high-protein diet.
-Maintain hydration – drink 6–8 glasses of water a day and avoid caffeine and alcohol.
-Stop smoking.
-Attend to basic principles of cleanliness and good personal hygiene and keep fingernails short.
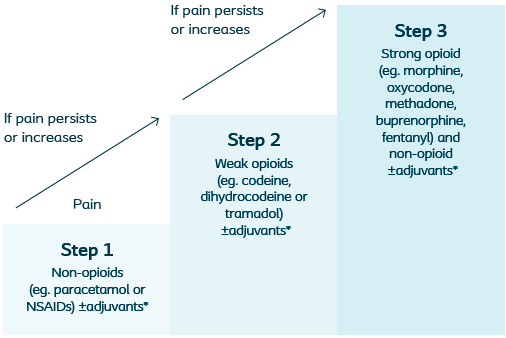
WHO Analgesic Ladder. *Adjuvants can be used along any step of the ladder, these may include antidepressants, anticonvulsants, corticosteroids and anxiolytics.
Research shows that patients who are included in planning their treatment and educated on effective self-care are more likely to adhere to their treatment plan. Learn more about how to include the patient and their caregivers in the Wound Care Pathway.
➔ The first dressing change should be 48 hours after injury and then every 3–5 days thereafter, depending on how healing is progressing.
To promote the goal of a shorter time to wound healing it is important to prevent the desiccation of viable tissue and control bacteria by choosing a dressing that promotes moist wound healing.

Cleansing and debridement

Hypertropic scar

Hypertropic scar
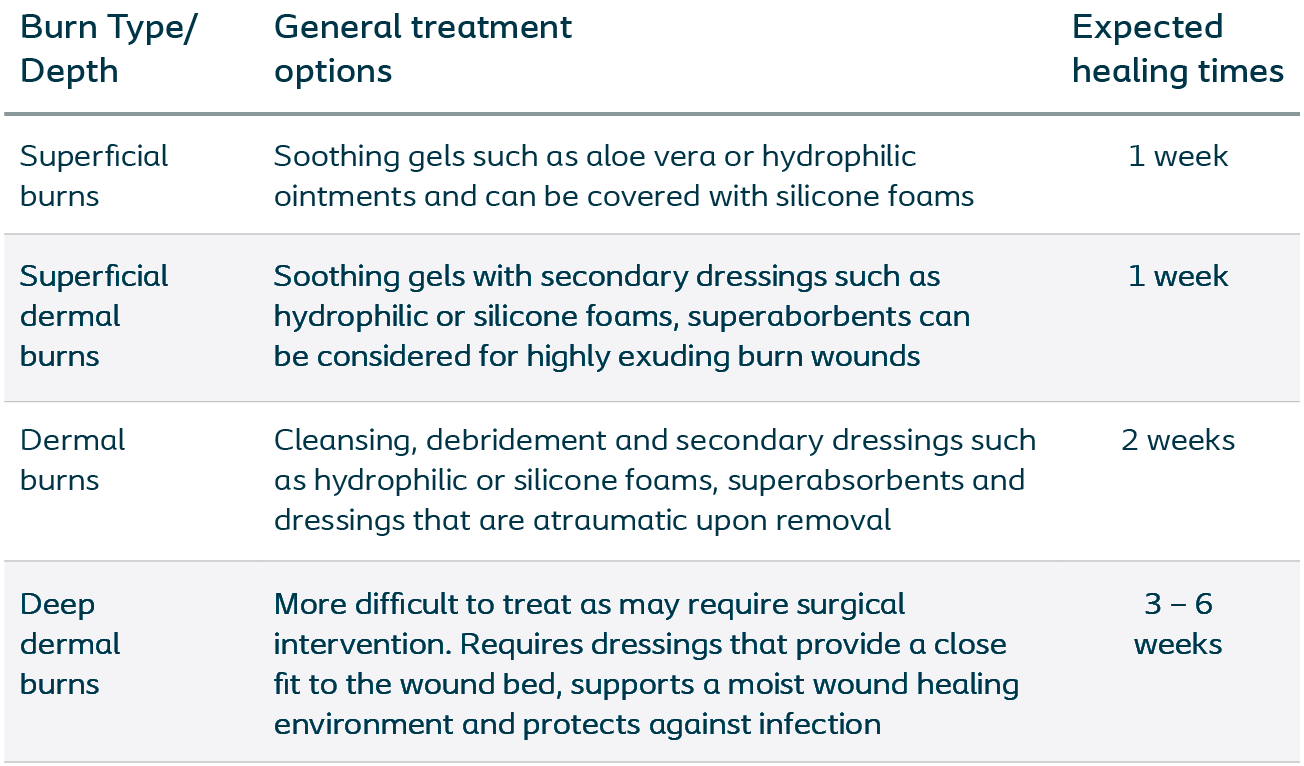
➔ A burn dressing should:
Dressing selection should be based on patient needs and preferences and local policy/protocol/formularies. The following chart breaks down some of the basic theory around dressing types and how they can help manage symptoms for patients with burn wounds.
➔ Always use an aseptic or non-touch application technique on application and removal.
➔ Ensure dressings do not impede patient mobility and are secured to avoid slippage
➔ Advise patients to keep dressing dry and clean.
➔ Dressing should be changed within 24–48 hours after initial injury and every 3–5 days thereafter, depending on how healing is progressing.
➔ Dressings should be changed immediately if they become painful, odorous, or saturated. It is important to remind patients to contact their care provider if any of these complications occur.
➔ Taking photos of the wound will help monitor healing progress and may be useful if specialist advice about assessment and treatment needs to be sought.
➔ If a non-complex burn wound has not healed in 2-weeks, refer.
➔ Monitor for complications, such as spreading infection or toxic shock syndrome, if suspected refer.
➔ Provide patients and caregivers with written information about the key stages of their management including wound care, pain & itch management and clear warnings signs as to when to seek additional care.
– the interval worsening or deepening of the depth of burn wounds over time, often seen in children due to their thinner dermis.
– drying of the wound bed which delays healing or ceases healing altogether.
– composed of necrotic skin destroyed by the burn, coagulated protein from the exudated plasma, and bacterial exudates which have begun developing. Normally the eschar loosens about the second or third week, and underneath the eschar the granulation base appears.
– occur when the burn scar matures, thickens, and tightens, preventing movement.
– swollen with an excessive accumulation of fluid.
– thick, irregular scarring that forms months to years after the inciting injury. Often shiny, hairless, lumpy, raised skin that is itchy and causes discomfort.
– An infection that is in the bloodstream is called a systemic infection. An infection that affects only one body part or organ is called a localised infection.
– there are 3 zones in injury in burns. The zone of coagulation is the tissue that was destroyed at the time of injury. The zone of stasis has a compromised blood supply, inflammation and tissue injury. The zone of hyperaemia sustains the least damage, where microvascular perfusion is not impaired. Often the area of stasis will progress and become necrotic within 48 hours following the injury.
For a glossary of general wound care terms consult The Wound Care Pathway: