
The Wound Care Pathway: Your 5 step guide to wound healing
PDF
6 MB
25
pages
By following the steps in this pathway, you can provide an optimal healing environment for malignant wounds and reduce the risk of complications that could lead to delayed healing or worse.
Any advice included here needs to work in conjunction with your local protocols and your individual scope of practice.
This article is based on the book A pathway for treating a person with a: Malignant wound.
Malignant wounds are predominantly cancer related, however, people at the end of life may present with malignant fungating wounds that are noncancerous in origin.1 Malignant wounds are challenging because of their typical characteristics – excessive leakage/exudate, bleeding, pain, malodour and disfigurement.2 Malignant wounds are also referred to as tumour necrosis, a fungating wound, ulcerating cancerous wound, malignant cutaneous wound, fungating wound, marjolin’s ulcers or malignant lesions. Malignant wounds are often end-of-life wounds that have a low potential for healing, making them challenging to treat and requiring a focus on symptomatic care, with the aim to improve quality of life (QoL).1
This pathway is focused on treating a person with a non-healing malignant wound. Patients with malignancy who have a wound of another ethiology should be treated using the pathway that best matches the wound’s originating ethiology. For example, for a patient with a surgical wound where a malignant tumour has been surgically removed please follow the Surgical Wounds Pathway or if a patient has a venous leg ulcer that turns malignant, but is deemed healable, it is best to follow the Venous Leg Ulcer (VLU) Pathway.
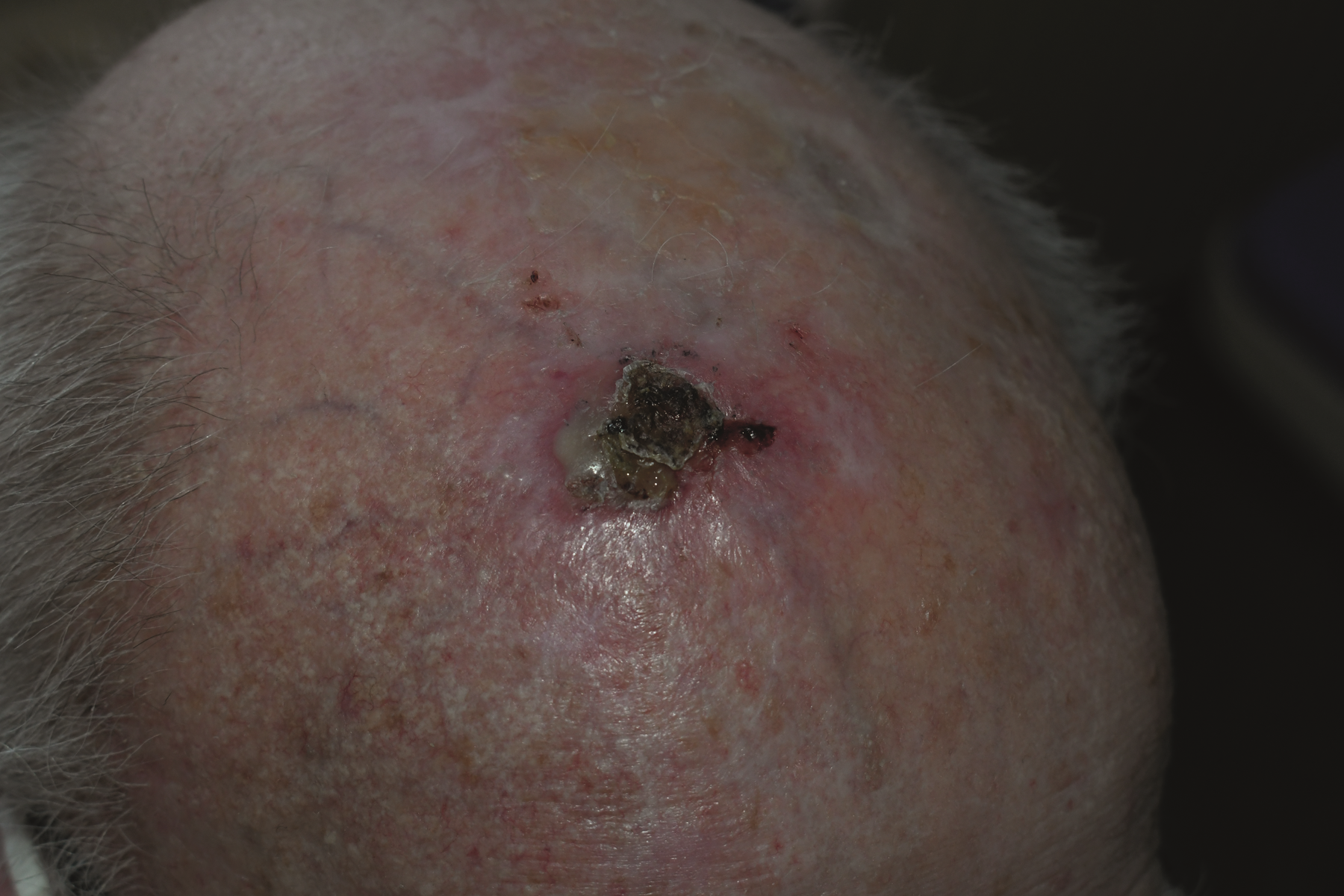
Squamous Cell Carcinoma

Basal Cell Carcinoma
Malignant Wounds can generate excessive suffering for the patient and their caregivers due to:3
Patients and their caregivers/families often require psychological, spiritual and emotional support along with physical care. The aim of malignant wound management is to reduce the devastating impact the wound has on the individual, their family and their care team, whilst acknowledging the potential for new wounds to develop as the carcinoma escalates or pressure injury/ulcers develop as the skin fails.1
➔ Conduct a holistic patient assessment with a focus on patient quality of life, social and family support/environment.
➔ Conduct a wound assessment using a validated assessment tool, with the following special considerations:
➔ Conduct a detailed pain assessment to determine the nature and type of pain, duration, severity and impact of daily living, etc. using a validated pain assessment tool.
➔ Include a complete physical exam to check for other injuries/complications (i.e. pressure injuries, skin failure, etc.), including a nutritional assessment as patients with malignant fungating wounds often have significant problems with appetite due to odour.
ALWAYS take the patient’s goals of care into account. With fungating malignant wounds, patient and caregiver’s primary concerns may not be wound treatment but other issues such as odour, pain and mobility restrictions/activities of living.
➔ Examples of patient care goals
1. Schedule regular holistic patient and wound reassessments based on the patient’s changing condition and situation.
2. All treatments should be patient driven. It is also important to ask the patient’s permission at each visit before conducting assessments, change dressings etc.
➔ Management of malignant wounds is complex and requires a multidisciplinary approach to care.
➔ Putting together a multidisciplinary/integrated care team is critical.
➔ The patient and their family/caregivers must be considered full and active members of the care team.
➔ The team should include everyone with a role in the patient’s clinical, psychological and spiritual care.
When putting together a multidisciplinary care team, flexibility is key. Additional team members may be required as the patient progresses and new specialised skills are needed, i.e. pain management specialist, hospice care, etc.
➔ Developing treatment goals
➔ SMART goals

SMART goals
➔ Treatment planning
- Use of aromatherapies (some scents may cause nausea for patients. A trial- and error approach to determining which if any scents help may be required).
- Keeping room well ventilated.
- Kitty litter under the bed.
➔ WHO Analgesic Ladder
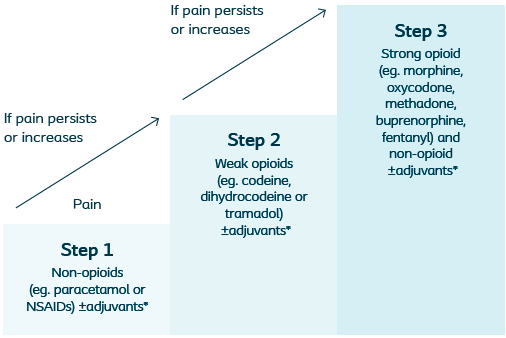
WHO Analgesic Ladder. *Adjuvants can be used along any step of the ladder, these may include antidepressants, anticonvulsants, corticosteroids and anxiolytics.
1. Many treatments for these patients lack higher level evidence due to the nature of this patient population. Often a trial-and-error approach to reducing symptoms is required to find the solution that works best for the patient and family caregivers.
2. Patient and family/caregiver education is paramount. Understanding expected disease progression, effective supported self-care options and preparing for contingencies (i.e. haemorrhages) allow patients and families/carers to be actively and appropriately involved in treatment planning.
➔ Cleansing & Debridement:

Basal Cell Carcinoma

Breast carcinoma
1. Decisions around therapeutic cleansing and debridement should always take into account patient comfort and care goals. Ask the patient if it is OK to cleanse the wound. If the patient declines, explain the benefits of the treatment, but if the patient does not want the treatment respect his/her wishes.
2. Avoid unnecessary manipulation of the wound, especially for patients with malignant end-of-life wounds
Localised inflammatory effects of the malignant wound may have many of the same characteristics as infection, such as appearing red, inflamed and warm to the touch.
➔ Dressing choice should always take into account current treatment and procedures that may impact dressing type and change frequency, such as radiotherapy.
➔ A dressing should manage exudate, prevent infection, protect periwound skin, allow the patient maximum mobility, comfort and security and be non-traumatic on application and removal.
➔ Non-adherent soft silicone dressings have been shown to cause less pain upon removal.2
➔ Choose a dressing that:
• Reduces infection risk and odour.
➔ Avoid the use of petroleum impregnated dressings and occlusive hydrocolloid dressings in fungating wounds.5
1. It is important to ask the patient’s permission at each visit before conducting a dressing change.
2. Avoid MARSI by using non-adhesive dressings and careful dressing removal.
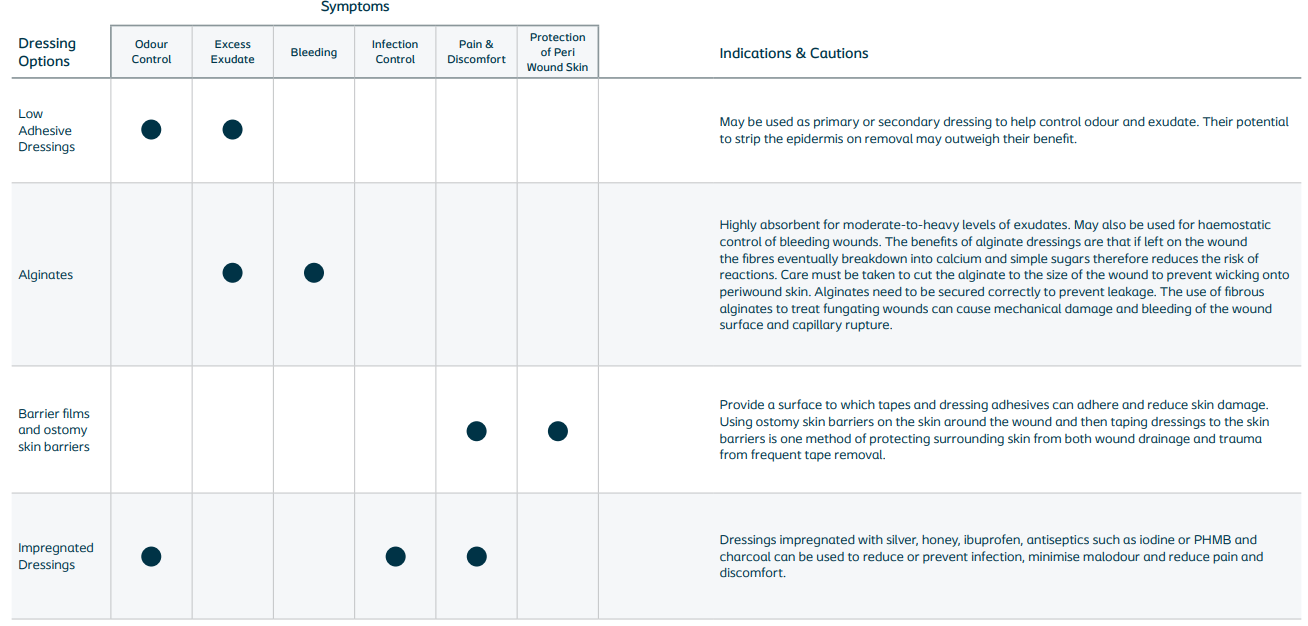
➔ Malignant wounds are often highly exudating and irregular in size and shape, which makes them difficult to dress and may require an unorthodox approach. A multiple layered dressing approach may be required. Dressing selection should be based on patient needs and preferences and local policy/protocol/formularies. The following chart (see below) breaks down some of the basic theory around dressing types and how they can help manage symptoms for patients with malignant fungating wounds.
If patient is not responding to standard care, consider referral for adjunct therapies such as:

➔ Care must be flexible and focused on the patient’s priorities, as well as management and control of symptoms.
➔ Assess progress towards care goals and acknowledge that the patient’s goals may change as their condition progresses.
➔ Taking photos of the wound at dressing changes can help assess progression and will allow other members of the care team to “see the wound” without disturbing the patient. Always ask patient permission before taking the photo and also ask patient if they would like to see the image.
➔ Monitor environment of care and openly discuss care options with patient and family/caregivers.
The patient should ALWAYS drive decision-making.
➔ Patient and care giver education and communication:
➔ Caregiver support

– A cancerous lesion involving the skin, which is open and may be draining. The lesion may be a result of a primary cancer, or a metastasis to the skin from local spread or local invasion. It may take the form of a cavity, an open area on the surface of the skin, skin nodules, or a nodular growth extending from the surface of the skin.12
– Sibbald (2009)15 defines end of life as a phase of life when a person is living with an illness that will often deteriorate and eventually cause death.
– when a tumour that is growing under the skin breaks through the skin’s surface and creates a wound. As the cancer grows, it can block and damage blood vessels, reducing oxygen supply to the surrounding skin and tissue causing necrosis.
– an unavoidable skin breakdown which occurs in some patients as part of the dying process.
– Medical Adhesive Related Skin Injury most often caused by the use of adhesives or the aggressive removal of dressings.
– a cutaneous malignancy that forms in the area of previously injured skin, burn scars, and chronic wounds.
– refers to itchy skin and can have cutaneous, neuropathic, neurogenic, or psychogenic origins.
– when passages or openings develop under or adjacent to the wound bed or there is erosion under the wound edges. Both tunnelling and undermining create cavities within the wound bed where exudate can pool and cause infection.
For a glossary of general wound care terms consult The Wound Care Pathway: