
The Wound Care Pathway - Your 5 step guide to wound healing
PDF
6MB
25
pages
By following the steps in this pathway, you can provide an optimal healing environment for surgical wound dehiscense and reduce the risk of complications that could lead to delayed healing or worse.
Any advice included here needs to work in conjunction with your local protocols and your individual scope of practice.
This article is based on the book A pathway for treating a person with a: Surgical wound dehiscence.
Surgical Wound Dehiscence is the separation of the margins of a closed surgical incision that has been made in the skin. It will sometimes involve an exposure or protrusion of underlying tissue, organs or implants. The separation may occur at a single or multiple regions, or involve the full length of the incision, and may affect some or all tissue layers.¹
The most common causes can be categorised as:
That a surgical wound dehiscence generally occurs between 4-14 days after surgery but can also occur up to 30 days after. A dehisced incision may, or may not, display clinical signs and symptoms of infection.1

Surgical wound dehiscence occuring at multiple regions

Surgical wound dehiscence involving full length of incision and affecting all tissue layers

Surgical wound dehiscence with exposure of underlying tissue and implant
The guidance provided in this Wound Type Specific Pathway, is best understood in combination with the detailed guidance available to you in The Wound Care Pathway.
➔ First, you should conduct a holistic patient assessment:
For more information on how to conduct a holistic patient assessment, look to The Wound Care Pathway.
➔ Next assess the dehiscence, by using a validated assessment tool like the Triangle of Wound Assessment:

Measure length and width of dehisced wound
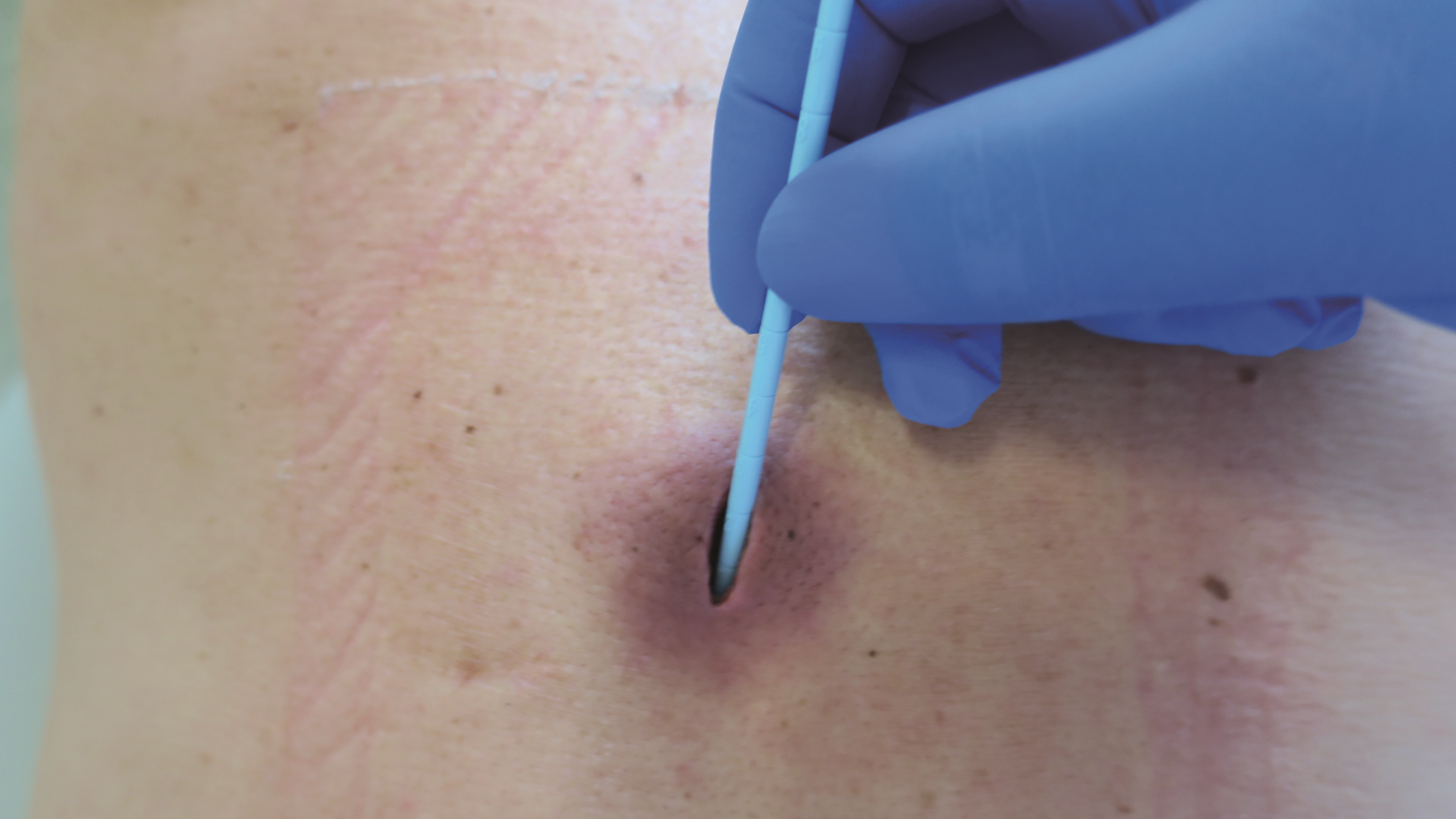
Probe to measure wound depth
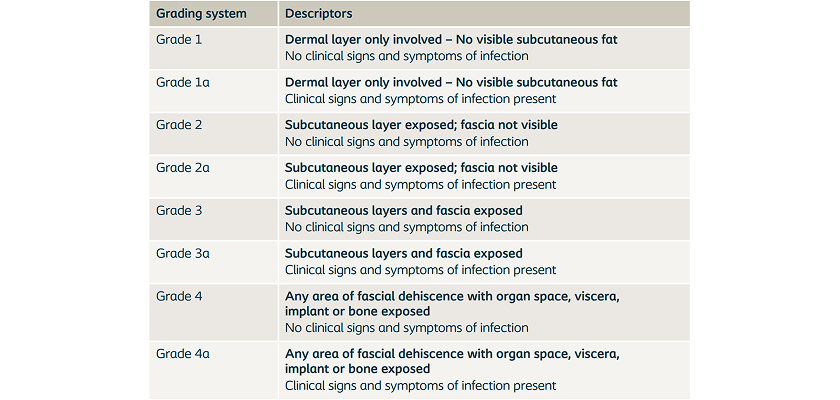
➔ Categorize the surgical wound dehisence (SWD) according to the WUWHS grading system from 1 / 1a, to 4 / 4a.¹
That with surgical wound dehiscence it is important to be aware of how signs and symptoms may present in a range of skin tones (i.e. colouration).
➔ First you should diagnose the severity of the dehisced surgical wound by grading it from 1/1a-4/4a.
➔ Then assess for signs of infection. You should check for infection by looking for:
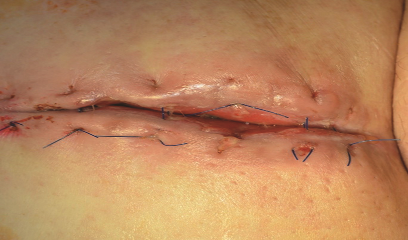
A dehisced surgical wound with no clinical signs of infection.

A dehisced surgical wound presenting several signs of infection; Pain, odor, redness and pus

Dehisced surgical wound presenting two common signs of local infection = Redness and oedema

➔ Always develop a holistic care plan that involves the patient in both development and implementation. Review patient expectations and outcomes and potential limitations.
➔ Let your treatment plan be determined by the severity of the dehiscence and the absence or prevalence of infection. If infection is already present you should treat the wound as a priority.
➔ Make sure you take all factors into account as you plan:
That signs of inflammation at the incisional site, e.g. warmth, erythema, oedema, discolouration and pain, are normal during the first few days after surgery, and do not necessarily indicate infection.
➔ First, prepare the wound bed by cleansing and debriding the wound to remove debris and necrotic or indolent tissue
➔ You should use every dressing change to assess the wound again. Use a validated assessment tool to conduct a formal reassessment on a regular basis until wound is fully healed
➔ Consider using NPWT for highly exudating wounds and for wound dehiscences, that are categorized as grades 3 & 4. As healing progresses, step down from advanced therapies (i.e. when exudate decreases or wound improves consider stepping down from NPWT to standard dressing).
For more information about managing infection, consult: Ten top tips: managing surgical site infections.
➔ To provide an optimal healing environment, choose a dressing that is appropriate for the level of exudate, size of wound and skin type. The dressing type may need to be changed as healing progresses, or if there is no progress in the wound over a two-week period.
➔ Make sure the dressing is able to conform to the wound bed – it should leave no gap between dressing and wound bed in order to effectively manage exudate, moisture and bacterial balance.

Wound bed conforming dressing used on surgical wound dehiscence

Wound bed conforming dressing used on surgical wound dehiscence

Gelling fiber used on a surgical wound dehiscence
➔ Only choose dressings that are atraumatic upon removal. You should be able to easily remove it intact, and not cause further damage to the wound bed or periwound skin.
➔ If you suspect infection use a dressing with antimicrobial properties.
If you are inserting more than 1 dressing, the number of dressings needs to be documented on the dressing or in the chart and all should be removed at the next dressing change.
➔ You should conduct reassessments at time intervals that are appropriate for the severity of wound.
➔ As part of your holistic care plan involve your patient in monitoring and managing the surgical wound dehiscence. Your patient education should include:
➔ Monitor for signs of oedema and manage swelling
➔ Assess vascular status if the dehiscence is on lower extremities.
➔ Consider a re-evaluation near end of the process to confirm healing and to evaluate scarring. Excess scar tissue can reduce mobility, delay return to normal activities and the visible aspect may affect the psychosocial wellbeing of the patient.2-4
Communication among care team members is paramount.

Wound with bone visible

Wound with implant visible

Wound with signs of spreading infection

Leg wound with signs of infection & ischemia

Leg wound with suspected ischemia
– is a liquid that oozes from a wound, often thick with a milky look and texture that can vary in colour, from grayish or yellow to green or brown
– are swollen areas within body tissue, containing an accumulation of dead white blood cells and bacteria with tissue debris and serum.
– are localized accumulations of serum fluid, occurring most commonly as a complication of a surgical procedure.
– is an abnormal collection of blood outside of a blood vessel, causing swelling. A bruise is bleeding under the skin without swelling. The skin over a haematoma often feels spongy, rubbery and lumpy. Severity of haematoma depends on the size and depth. Refer patients if the haematoma is large, tense, painful, infected, over a joint or airway or is expanding.
– a build-up of fluid which causes the affected tissue to become swollen and can be localized or more general.
For a glossary of general wound care terms consult The Wound Care Pathway: