
The Wound Care Pathway: Your 5 step guide to wound healing
PDF
6MB
25
pages
By following the steps in this pathway, you can provide an optimal healing environment for venous leg ulcers and reduce the risk of complications that could lead to delayed healing or worse.
Any advice included here needs to work in conjunction with your local protocols and your individual scope of practice.
This article is based on the book A pathway for treating a person with a: Venous leg ulcer.
A venous leg ulcer is an open, often painful, sore in the skin on the leg below the knee. The ulcers usually develop on the inside of the leg and take more than 2 weeks to heal.
Most common cause:
Venous leg ulcers are caused by venous hypertension, such as chronic venous insufficiency.1,2,3,4
Characteristics:
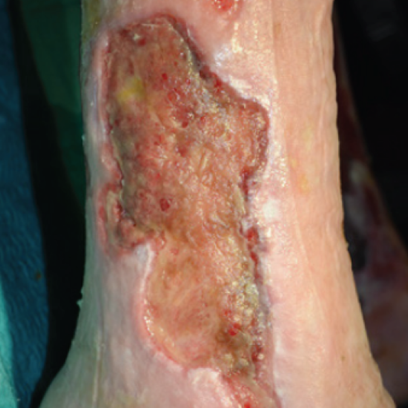
A venous leg ulcer usually presents as a shallow ulcer with irregular margins and appears over the area of atrophic and/or pigmented skin. Visit this link to learn more about venous leg ulcers.

Venous leg ulcer on the lower leg
Venous leg ulcer on the lower leg

Venous leg ulcer on the lower leg
The guidance provided in this Wound Type Specific Pathway, is best understood in combination with the detailed guidance available to you in The Wound Care Pathway.
➔ Begin with a holistic patient assessment.
• For more information on how to conduct a holistic patient assessment, look to The Wound Care Pathway.
➔ Proceed with a lower limb assessment using a validated assessment tool (i.e. Leg Ulcer Measurement Tool LUMT).
➔ Then begin your wound assessment using a validated wound assessment tool (i.e. Triangle of wound assessment).
• Make note of wound size, wound bed, amount and type of exudate, condition of wound edge and periwound skin and signs of infection
• Also check position of the ulcer – malleolus or gaiter area
➔ Make your assessment by checking for oedema and looking for:

Maceration

Stasis dermatitis

Lipodermatosclerosis

Hyperkerastosis
Learn more about Hyperkeratosis of the lower limb.
When you are looking for ulceration in a leg, all changes in the skin (including colour and texture should be thoroughly assessed.)5
➔ Be sure to check for signs of venous insufficiency, by looking for:
• Oedema – measure circumference of ankle, foot and calf.
• Signs of vascular insufficiency – inspect arterial flow and perfusion.
• Signs of venous hypertension – inspect legs for varicose veins – (reticular phlebectasia), skin changes (i.e. small widened blood vessels (telangiectasia), and changes in pigmentation.
In the case of venous disease, lipodermatosclerosis and haemosiderin staining are easier to see in pale skin. For patients with dark skin tones feel for the hardening in the skin and compare the affected leg to the other leg for comparison of colour and swelling.5
➔ You should also consider:
• Patient’s BMI (Body Mass Index) – a BMI of between 53-59 is usually when lymphedema occurs.6
• Other risks and complicating factors such as: patient mobility, prolonged sitting or standing, calf muscle pump, gait, comorbidities, medications, family history, etc.
➔ When you are dealing with a venous leg ulcer, it is important to also diagnose the leg to exclude arterial insufficiency.
➔ Use the ABPIs (Ankle Brachial Pressure Index) as a means of differential diagnosis and to assess the leg for ischemia.7 (At a minimum, pulse palpation is mandatory – follow local policy)
➔ Be sure to measure pulse on both locations on the ankle – posterior tibial artery and dorsal pedal artery.

Explore pulse at multiple locations on ankle and foot without gloves

• If you measure no pulse in both locations on the ankle
• If you don’t know whether it is venous or arterial ulcer, or an unknown aetiology
• If you are unsure of the diagnosis or the Doppler does not match the presenting signs and symptoms
People with diabetes can have calcification which means their ABPI can be falsely elevated.8 Caution should be exercised with this group. If wave forms on Doppler are biphasic or triphasic and pulse is palpable, it is generally safe to apply compression therapy. In case of ABPI >1.3 or if there are discrepancies between ABPI and clinical signs refer.
➔ Once your diagnosis of the leg has excluded arterial insufficiency, you are ready to determine the need for any additions to the standard treatment planning procedure.
➔ You should proceed according to the result of your ABPI:
• In case your ABPI is more than 0.8, arterial, involvement can be ruled out and compression therapy can be considered at 40mmHg.
• In case your ABPI is between 0.5 and 0.8 refer for advice regarding level of compression.
• In case your ABPI is less than 0.5 do not compress and refer immediately for vascular assessment.
Discover our free online medical education programme supporting clinicians who are managing wounds and skin care complications.
➔ First, prepare the wound bed by cleansing and debriding the wound to remove debris and necrotic or indolent tissue. Cleansing of the full leg with a pH-appropriate cleanser is recommended to reduce odour and to protect the skin surrounding the ulcer. If possible get the patient to shower.
➔ Be prepared to manage exudate to protect the periwound skin, as venous leg ulcers are often highly exudating. (This will reduce over time with the correct level of compression therapy).
➔ Frequently undertake a patient reported pain assessment, as leg ulcers are ranked as the most painful compared to other wounds.2
➔ Apply compression therapy for patients with active venous ulceration and an ABPI above 0.8 – and refer for vascular assessment and monitoring. (Compression therapy aims to improve venous return and reduce venous hypertension. Compression is usually graduated and can include bandages, wraps, calf pumps and compression hosiery.)1,8
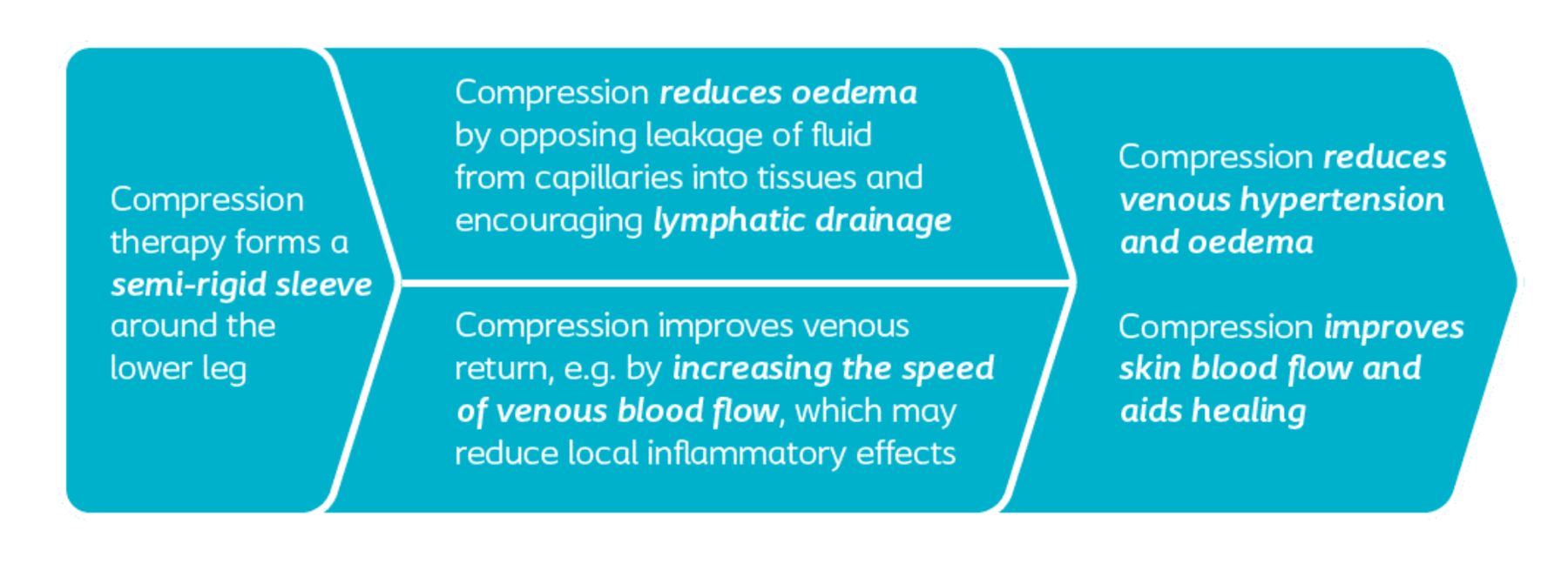
The concept of compression therapy
➔ Choose the correct type of compression by taking relevant factors into account: The severity of the disease, the anatomical characteristic of the leg/ankle, required frequency of applications, and the functionality of the patient: Patient preference, mobility, lifestyle and likely concordance.9
➔ Check for signs of infection at each dressing change, as infection and biofilm are common in venous leg ulcers. Use the IWII infection continuum and management guide.
➔ Choose a dressing that helps you effectively manage exudate, as venous leg ulcers are typically highly exudating.
➔ Make sure the dressing is able to conform to the wound. It should leave no gap between dressing and wound bed in order to effectively manage exudate and bacterial balance. For highly exuding wounds consider a superabsorbent dressing.

➔ Look for dressings that are atraumatic upon removal – it should not cause further damage to the wound bed or periwound skin – but should ideally help decrease pain and odour for patients.
➔ If you suspect infection use a dressing with antimicrobial properties.
➔ Consider adjunct therapies like NPWT when appropriate.
➔ You should monitor venous leg ulcers at least every 4 weeks. Specifically look for distortion or modification of the shape of the leg.
➔ Measure oedema reduction or redistribution at every dressing change and action taken as needed to amend the compression regime.
➔ In case, the wound is not healing with therapeutic compression refer to a vascular specialist, if that has not already been done.
➔ In case ulcer has not healed after 12 weeks, reassess differential diagnosis. Also revisit holistic patient assessment to assess if factors such as low haemoglobin, immune function deficits or other co-morbid conditions are affecting healing. You should also re-consider other risk factors such as patient’s lifestyle, past compression usage, etc.
➔ Discuss prevention strategies with patient such as skin care, life long compression hosiery, physical exercise (ankle & dorsal reflection, gait, calf muscle pump), weight control, etc.
For patients with healed venous leg ulcers, long term compression should be considered to reduce the risk of recurrence.
Also refer in case you...
– is a condition in which the veins fail to return blood efficiently to the heart. Symptoms include swelling of the legs and pain in the extremities.
– is a build-up of fluid which causes the affected tissue to become swollen and can be localized or more general.
– is a lack of blood supply to a certain part of the body, which may cause tissue damage due to lack of oxygen and nutrients.
– occurs when skin is in contact with moisture for too long. Macerated skin looks lighter in colour and wrinkly and may feel soft or soggy to the touch.
– is when there is venous insufficiency, or poor circulation in the lower legs, leading to skin discoloration, pain, itching and sores.
– is a chronic inflammatory condition characterised by subcutaneous fibrosis and hardening of the skin on the lower legs.
– is a thickening of the skin’s outer layer.
– is a brown iron-containing pigment usually derived from the disintegration of extravasated red blood cells.
– the region of the leg located circumferentially around the lower leg from approximately mid-calf to just below the ankle.
For a glossary of general wound care terms consult The Wound Care Pathway: