
Get full access with a free account
Benefits of the Coloplast® Professional Educational platform
Get full access to all educational content, events and resources
Track your progress
Share content with your collegues
Share supporting material with your patient
The role of the skin in wound healing
The skin’s structure plays a crucial role in wound healing. So, when we want to assess and manage wounds effectively, it’s important that we understand how the skin structure works.8
In this section, you’ll learn about:

How does the skin work?
The skin’s most important function is to protect our body from harm.
For example, the skin protects us from trauma, toxins, ultraviolet light and microorganisms. It also keeps us from getting dehydrated and helps our body maintain the right temperature.8,18
In the next section, we examine the three different layers of skin – what each layer does and why it’s important.
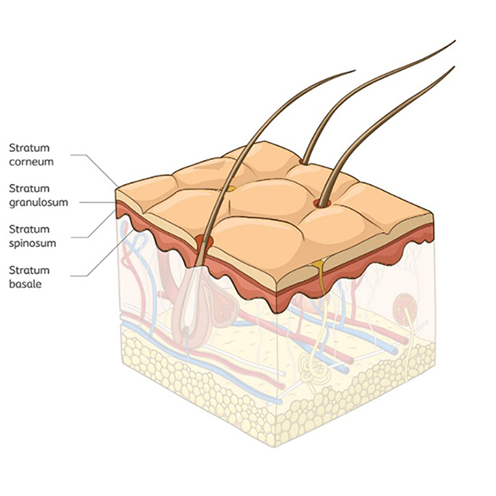
The epidermis
This layer of skin is made up of four layers. The top layer, the stratum corneum, is renewed about every 15 days in individuals with healthy skin.
What does it do?
The epidermis has three types of cells, each with a specific function:
- Keratinocytes
The majority of the cells in the epidermis (95%) are keratinocytes. These cells retain moisture, which helps the skin act as a barrier.33 - Melanocytes
These cells give skin its colour, or pigment. They also protect the skin from ultraviolet (UV) light.33 - Langerhans cells
These cells are a part of the immune system. They protect the body from potential allergens, bacteria and toxic substances by triggering an immune response.10,33
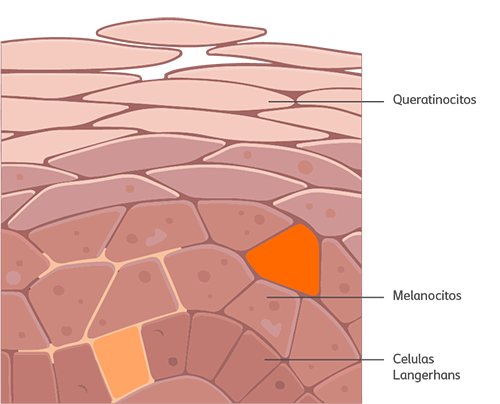
The three types of skin cells in the epidermis
These cells each play a role in the epidermis’ three vital functions:
- to act as a barrier;
- to control water loss; and
- to protect our bodies from UV light, bacteria and allergens.18
Why is it important?
The epidermis is a highly specialised structure that adapts to the world around us. It provides a physical and chemical barrier that protects the body by:
- preventing foreign substances from entering the body; and
- triggering the body’s immune system when any pathogens break through the barrier.18,26
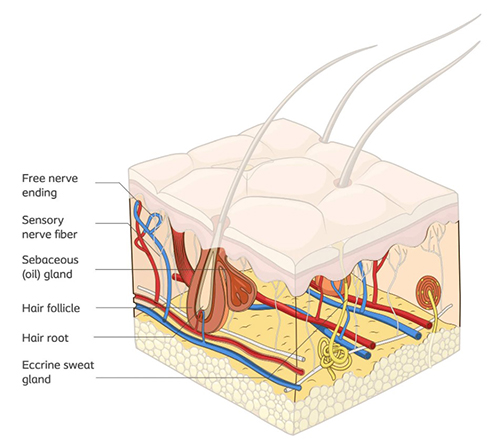
The dermis
What is it?
The dermis is the middle layer of the skin. It’s approximately 15-40 times thicker than the epidermis. The dermis contains nerve endings; blood vessels; and skin appendages, such as hair follicles, sebaceous glands and sweat glands.4,33
The dermis
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
What does it do?
The dermis is responsible for many of the skin’s important functions. For example, it’s where we feel sensation, such as pain and temperature.
The dermis also contains the glands that secrete sebum, which helps the skin maintain the right moisture balance. And sebum and sweat combine to create an acidic environment on our skin, known as the “acid mantle”.33
Why is it important?
The dermis plays an important role in maintaining the skin’s moisture and pH balance. This balance helps to prevent infection. In full-thickness wounds (wounds, such as pressure injuries (link to section ), that penetrate all three skin layers), the dermis is lost. That’s why these wounds take a long time to heal because the tissue repair process is so complex.19,25 Once they do heal, the structures within the dermis, such as the sweat glands and hair follicles, are permanently lost.25

Did you know?
When a wound heals, the dermis doesn’t have the same structure and function as it does in undamaged skin. This is because the dermis is replaced by scar tissue, as you can see in this image.25
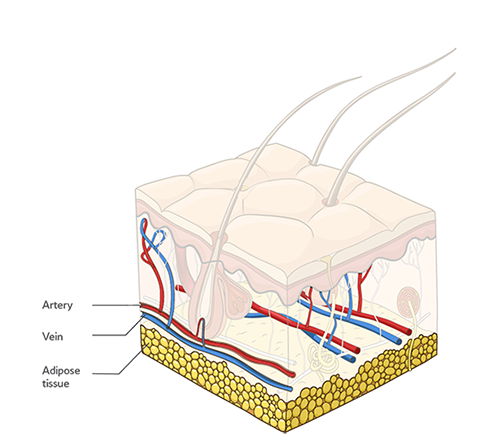
The subcutaneous tissue
What is it?
The subcutaneous tissue, also known as subcutis, is the lower layer of the skin. This layer contains connective and fatty tissue as well as major blood vessels and nerves.33 The thickness of the subcutis depends on several factors, including where it is on the body and the person’s age.
The subcutaneous tissue
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua.
What does it do?
The subcutis insulates our bodies. It acts as a cushion, protecting the internal organs from external pressure. It also plays a role in helping the body retain moisture.33
Why is it important?
The subcutaneous tissue is essential precisely because of its role in insulating and padding the body. In this way, it works to protect our bones, muscles, and the organs under the skin from physical damage.
If you want to learn more about how the skin is structured, watch this video [insert active link]
Did you know?
You’ll often be able to see the subcutis at the base of deep wounds, like pressure injuries or traumatic wounds.5
Four factors that affect the integrity of the skin
As we’ve discussed, the skin acts as a protective barrier for the body. It’s a dynamic structure that can adapt to environmental conditions. However, changes to the skin can weaken the barrier and leave the body open to infection.
In this section, we’ll take a look at the four most important factors that can affect the skin barrier.
Factor #1: Damage to the epidermis
The epidermis plays an important role in keeping out harmful substances. However, if the skin becomes dehydrated, the cells in the epidermis shrink. This causes the epidermis to crack, which breaks down the skin barrier. Harmful substances can then enter the body through those cracks. The skin can lose its ability to retain moisture, and the epidermal barrier can be damaged.18 (See image 5)
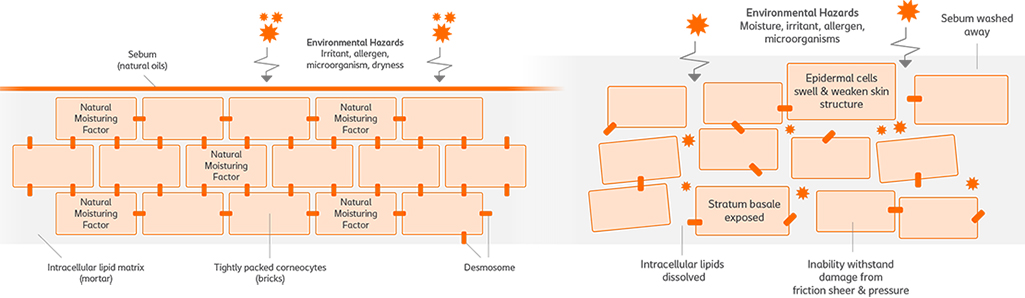
Image 5: This illustration shows you the difference between a healthy epidermis (on the left) and a damaged epidermis (on the right). If the epidermal cells break down, harmful substances can enter the body.

Factor #2: Age
Aging affects all three skin layers in the following ways:
- The epidermis barrier function declines, making the skin more vulnerable.18
- As we get older, the amount of collagen and elastin fibres in our skin reduces. This makes the dermis thinner, which decreases skin elasticity and increases the risk of skin tears.2,18
- The subcutis also gets thinner as we age. This means we have less protection against mechanical injuries. Our cells don’t reproduce as quickly, and the rate of sebum secretion decreases as well. All of this leads to delayed healing and an increased risk of infection.18,27
Factor #3: pH levels
As we discussed in the previous section, the skin’s acid mantle helps to maintain the right pH balance on the skin. This, in turn, keeps bacteria levels low.18,33 The skin’s acidic pH, humidity and natural cleansing processes all help to maintain the skin’s barrier function and integrity.18 If the skin loses its acidity, this can make the skin vulnerable to damage and infection.18
Factor #4: Moisture
Maintaining the right moisture balance in the skin is important part of preserving the skin’s integrity. If the skin is too moist or too dry, it can damage the epidermis. For example, dry skin often itches. Scratching dry skin can damage the skin’s protective barrier. Dry skin also negatively affects the skin’s pH balance (see Factor #3 above). The combination of these factors increases the risk of skin infection.29
At the other extreme, exposing the skin to too much moisture for an extended period of time can cause ‘moisture-associated skin damage’ (MASD). MASD decreases the skin’s ability to protect the body.
This is one of the reasons why it’s is important to manage the level of moisture in a wound. To learn more about how to do that, visit the exudate management section.
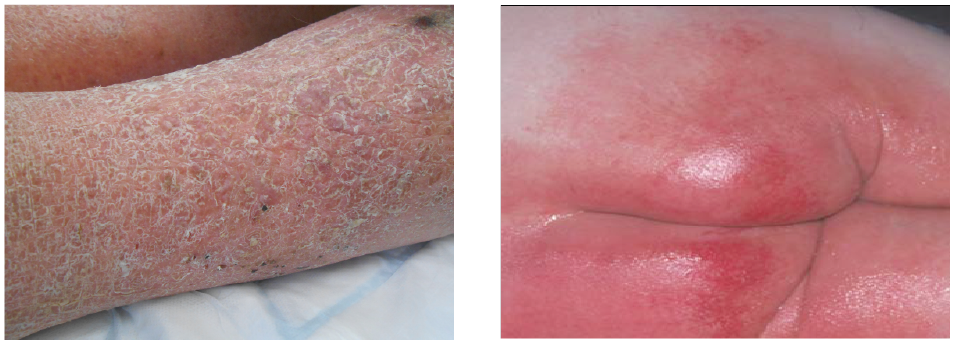
Dry skin Incontinence Associated Dermatitis
References
- Adderley, U. J. (2010) Managing wound exudate and promoting healing. British Journal of Community Nurses, 15(3), 15-20.
- Baranoski, S., Ayello, E., Tomic-Canic, M. (2008). Chapter 4: Skin: An essential organ. In Baranoski, S.(Editor) and Ayello, E. (Editor). Wound Care Essentials. Practice Principles (pp. 47-63). 2nd ed. Philadelphia: Lippincott Williams & Wilkins.
- Babb-Tarbox, M., Bergfeld, W. F. (2008). Chapter 11: Alopecia and Thyroid Disease. In Heymann, W. R. (editor). Thyroid Disorders with Cutaneous Manifestations (pp. 499-528). London: Springer.
- Baroni, A., Buommino, E., De Gregorio, V., Ruocco, E., Ruocco, V., Wolf, R. (2012). Structure and function of the epidermis related to barrier properties. Clinics in Dermatology, 30; 257-262.
- Beeckman, D., Schoonhoven, L., Fletcher, J., Furtado, K., Gunningberg, L., Heyman, H., Lindholm, C., Paquay, L., Verdú, J. and Defloor, T. (2007). EPUAP classification system for pressure ulcers: European reliability study. Journal of Advanced Nursing, 60(6); 682-691.
- Black, J. M., Gray, M., Bliss, D. Z., Kennedy-Evans, K. L., Logan, S., Baharestani, M. M., Colwel, J. C., Goldberg, M. and Ratliff, C. R. (2011). MASD Part 2: Incontinence-Associated Dermatitis and Intertriginous Dermatitis. Journal of Wound Ostomy & Continence Nursing, 38(4); 359-370.
- Brown, A., Flanagan, M. (2013). Chapter 4: Assessing Skin Integrity. In M. Flanagan (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 52-65). West Sussex: John Wiley & Sons, Ltd.
- Burian, E. A. (2017). Chapter 1: Huden. In B. Ø. Melby (editor), Bermark, S. (Editor). Sår og sårbehandling. En grundbog I sygeplejen (pp12-27). Copenhagen: FADL's Forlag.
- Chamlin, S. L., Tremblay, E. A. (2010). Chapter 1 You and the Skin You’re In. In Living with Skin Conditions (pp 1-13). New York: Facts on File, Inc.
- Ersser, S. J., Getligge, K., Voegeli, D. and Regan, S. (2005). A critical review of the inter-relationship between skin vulnerability and urinary incontinence and related nursing intervention. International Journal of Nursing Studies, 42; 823-835.
- Grove, G. L., Zerweck, C., Pierce, E. (2002). Chapter 23: Noninvasive Instrumental Methods for Assessing Moisturizers. In Leyden, J. J. (editor), Rawlings, A. V. (editor). Skin Moisturization (pp. 499-528). Boca Raton: CRC Press.
- Harding, C. R., Watkinson, A., Rawlings, A. V. (2000). Dry skin, moisturization and corneodesmolysis. International Journal of Cosmetic Science, 22; 21-52.
- Janninger, C. K., Schwartz. R. A., Szepietowski, J. C., Reich, A. (2005). Intertrigo and Common Secondary Skin Infections. American Family Physician, 72 (5); 833-8.
- Johnson, A. W. (2002). Chapter 1: The Skin Moisturizer Marketplace. In Leyden, J. J. (editor), Rawlings, A. V. (editor). Skin Moisturization (pp. 1-30). Boca Raton: CRC Press.
- Joshi R. Immunopathogenesis of psoriasis. Indian J Dermatol Venereol Leprol 2004;70:10-2
- Kennedy, R., Crowle A. (2017). Key Differences in Infant Skin. The Royal Children’s Hospital Melbourne. March 2017.
- Korting, H. C. (1990). Marchionini's Acid Mantle Concept and the Effect on the Skin Resident Flora of Washing with Skin Cleansing Agents of Different pH. In Braun-Falco, O., Flanagan, M. (Editor), Korting, H. C. (Editor). Skin Cleansing with Synthetic Detergents (pp. 87-96). Berlin: Springer-Verlag.
- Langøen, A. and Bianchi, J. (2013). Chapter 2: Maintaining Skin Integrity. In Flanagan, M. (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 18-32). West Sussex: John Wiley & Sons, Ltd.
- Lokmic, Z., Musyoka, J., Hewitson, T. D., Darby, I. A. (2012). In Jeon, K. W. International Review of cell and molecular biology, volume 296 (pp 140 - 173). Oxford: Elsevier Inc.
- Lumbers, M. (2018). Moisture-associated skin damage: cause, risk and management. British Journal of Nursing, 27 (12); 6-14.
- Mahoney, M., Rozenboom, B., Doughty, D. and Smith, H. (2011). Issues Related to Accurate Classification of Buttocks Wounds. Journal of Wound Ostomy & Continence Nursing, 38(6), 635-642.
- Martin, M. (2013). Chapter 3: Physiology of Wound Healing. In Flanagan M. (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 33-51). West Sussex: John Wiley & Sons, Ltd
- Muldoon (2013). Chapter 10: Chronic Ulcers of the Lower Limb. In Flanagan M. (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 155-174). West Sussex: John Wiley & Sons, Ltd
- Norman (2008). Chapter 12: Xerosis and Pruritus in the Elderly – Recognition and Management. In Norman, R. A (Editor), Diagnosis of Aging Skin Diseases (pp 151). London: Springer
- Paul, C. N. (2008). Skin Substitutes in Burn Care. Wounds Research, 20 (4).
- Proksch, E., Brandner, J. M. and Jensen, J-M. (2008). The skin: an indispensable barrier. Experimental Dermatology, 17; 1063-1072.
- Raschke, C. and Elsner, P. (2010). Chapter 5: Skin Aging: A Brief Summary of Characteristic Changes. In M. A. Farage, K. W. Miller and H. I. Maibach (Eds.), Textbook of Aging Skin (pp. 37-43). Berlin: Springer Berlin Heidelberg.
- Rawlings, A. W., Harding, C. R., Watkinson, A. Scott, I. R. (2002). Chapter 6: Dry and Xerotic Skin Conditions. In Leyden, J. J. (editor), Rawlings, A. V. (editor), Skin Moisturization (pp. 119-144). Boca Raton: CRC Press.
- Rosser, M., Couldridge G., Rosser, S. (2012). Body Massage. 3rd ed. Ocon: Bookpoint.
- Saffle, J. R., Banister, M., Cahalane, M., Lee, J. O., Palmieri, T. L. (2013). Chapter 10: Burns. In Lawrence, P. F. Essentials of General Surgery (pp. 188). 5th ed. Philadelphia: Lippincott Williams & Wilkins.
- Schmid-Wendtner, M-H., Korting, H. C. (2006). The pH of the Skin Surface and Its Impact on the Barrier Function. Skin Pharmacology and Physiology, 19; 296-302
- Sherwood, L. (2012). Chapter 11: The Blood and Body Defenses. In Sherwood, L. Fundamentals of Human Physiology (pp. 383). 4th ed. Belmont: Brooks/Cole.
- Shimizu, H. (2017). Chapter 1: Structure and function of the skin. In Shimizu, H. Shimizu’s Dermatology (pp 1- 42). 2nd ed. West Sussex: John Wiley & Sons, Ltd.
- Shimizu, H. (2017). Chapter 15: Disorders of keratinization. In Shimizu, H. Shimizu’s Dermatology (pp 1- 42). 2nd ed. West Sussex: John Wiley & Sons, Ltd.
- Sibbald, R. G., Kelley, J., Kennedy-Evans, K. L., Labrecque, C., Waters, N. (2013). A Practical approach to the Prevention and Management of Intertrigo, or Moisture-associated Skin Damage, due to Perspiration: Expert Consensus on Best Practice. Wound Care Canada, 11 (2); 1-21.
- Voegeli, D. (2012). Moisture-associated skin damage: aetiology, prevention and treatment. British Journal of Nursing, 21(9), 517-521.
- White, R. J. and Cutting, K. F. (2003). Interventions to avoid maceration of the skin and wound bed. British Journal of Nursing, 12(20), 1186-1201.
You may also be interested in…

HEAL e-learning
Learn about the function and structure of the skin with this EWMA-endorsed course.


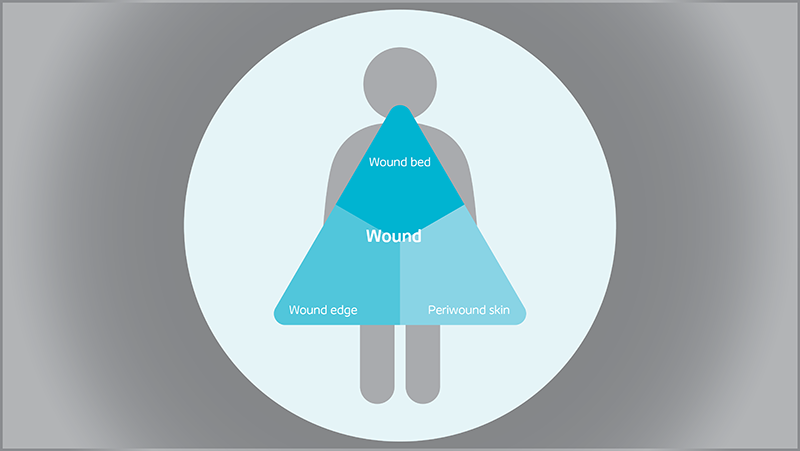
Triangle of Wound Assessment
Conduct a holistic and systematic wound assessment with our tool.