
Understanding moist wound healing
In this section, you’ll learn about:
What is a moist wound healing environment?
Thereare three types of wound healing environments:
- Dry - where the dressing absorbs, but doesn’t keep any of the moisture.
- Moist - where the dressing absorbs and keeps some of the moisture.
- Wet - where you seal the wound with an impermeable membrane that keeps all of the fluid within the dressing.18
Up until the 1960s, the most common approach to wound healing was to create a dry wound environment. Healthcare professionals either left the wound uncovered to allow it to dry, or they covered the wound with a dry gauze dressing.7
However, around that time, Dr. George D. Winter discovered something interesting. Superficial acute wounds healed twice as fast in a moist environment than under a dry scab.9 Since Dr. Winter’s discovery, clinical research has demonstrated that moist and wet dressings are far more effective than dry dressings in helping chronic wounds heal.10
Moist wound healing:
- prevents tissue dehydration and cell death;18
- reduces the risk of wound infection;12,19
- results in less scar tissue;19 and
- speeds up angiogenesis and epithelisation.18
Let’s see why that is.

Why do moist wounds heal faster?
Themain reason why moist wounds heal faster is that epithelial cells migrate faster in a moist environment.
In the final stages of wound healing, epithelial cells migrate across the surface of the wound to close it.5,6 These cells need moisture to move across the surface of the wound. If the wound environment is dry, the cells will have to find moisture deep in the wound bed so that they can migrate. This slows down the healing process.7 In fact, studies show that moist wounds heal 50% faster than dry wounds. If a wound is exposed to the air, it creates a dry environment that actually promotes cell death, not healing.4
Wound exudate, or fluid, also plays a vital role in the healing process. This fluid provides the nutrients, proteins, glucose and white blood cells that are necessary for the wound to heal. For example, neutrophils, a type of white blood cell, help protect the body from harmful microorganisms. In this way, exudate actually helps prevent wound infection.
This helps to explain why creating an optimal moisture balance around the wound is so important when managing chronic wounds.
How to create a moist wound healing environment?
Oneof the most important ways to create a moist wound healing environment is to choose the right type of dressing for the wound.
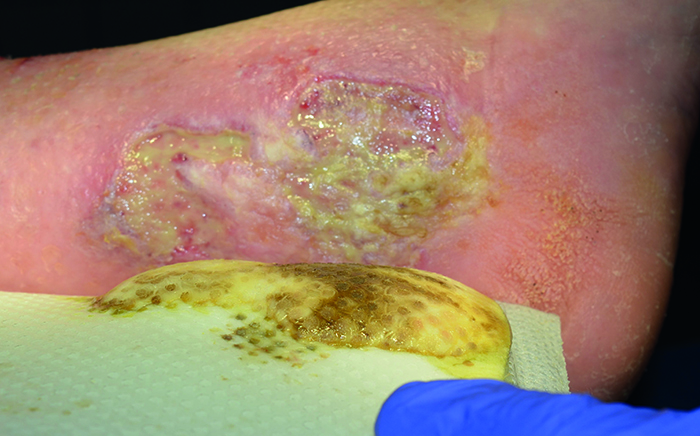
To find out which dressing you should choose, start by assessing the wound and the level of exudate. This assessment will give you the information you need to choose the right dressing and determine how often you need to change it.27
In general, you should look for a dressing that:
- removes excess exudate from the wound bed;
- protects the wound edges and periwound skin;
- maintains a moist healing environment;
- helps your patient feel confident and secure; and
- is easy for the patient to remove and care for.27
Choosing a moist healing dressing also eases the burden on your patient. When you use moist wound healing, removing the dressing is less painful and traumatic than with dry dressings.18,19 You don’t have to change the dressing as often, and you improve the healing time – all of which benefits the patient.20
Did you know?
Research shows that using moist wound healing dressings is far more cost-effective than traditional gauze-type dressings.20

When not to use moist wound healing
Keepin mind that moist wound healing is not suitable for all types of chronic wounds.
For example, you should be careful when using moist dressings on patients with gangrenous diabetic foot ulcers.15 This is because dry gangrene can progress to wet gangrene when moisture gathers under the dressing. You should also be careful if you’re using a moist dressing on a patient with a malignant fungating wound covered by a dry scab (eschar). In these cases, the scab can help to stabilise the wound.17
What about wet-to-dry dressings?
Research shows that wet-to-dry and dry adherent gauze dressings are not effective in wound healing.21 Wet-to-dry dressings debride the wound by ripping tissue from the wound’s surface.22,23 This method:
- damages granulation tissue and causes bleeding;24
- causes pain when removing the dressing;21,22,24
- increases the risk of infection;22
- spreads infection in colonised wounds during dressing change;22,25 and
- dehydrates the wound bed.23
References
- Gottrup, F., Apelqvist, J. and Price, P. (2010). Outcomes in controlled and comparative studies on non-healing wounds: recommendations to improve the quality of evidence in wound management. Journal of Wound Care, 19(6), 239-268.
- Flanagan, M. (2013). Chapter 5: Principles of Wound management. In M. Flanagan (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 66-86). West Sussex: John Wiley & Sons, Ltd.
- Queen, D., Harding, K. (2013). Chapter 17: Dressings: The Healing Revolution. In M. Flanagan (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 278-90). West Sussex: John Wiley & Sons, Ltd.
- Field, C. K., Kerstein, M. D. (1994). Overview of Wound Healing in a Moist Environment. American Journal of Surgery, 167(1AS) 2S-6S
- Dyson, M., Young, S., Pendle, C. L., Webster, D. F. and Lang, S. M. (1988). Comparison of the effects of moist and dry conditions on dermal repair. The Journal of Investigative Dermatology, 91(5),
- Vogt, P. M., Andree, C., Breuing, K., Liu, P. Y., Slama, J., Helo, G. and Eriksson, E. (1995). Dry, Moist, and Wet Skin Wound Repair. Annals of Plastic Surgery, 34(5), 493-500.
- Baranoski, S., Ayello, E. (2012). Wound Dressings: An Evolving Art and Science. Advances in Skin and Wound Care, 25:87-92
- Madden, M. R., Nolan, E., Finkelstein, J. L., Yurt, R. W., Smeland, J., Goodwin, C.W., Hefton, J. and Staiano-Coico, L. (1989). Comparison of an occlusive and semi-occlusive dressing and the effect of the wound exudate upon keratinocyte proliferation. The Journal of Trauma, 29(7), 924-931.
- Winter, G. D. (1962). Formation of the scab and the rate of epithelialization of superficial wounds in the skin of the young domestic pig. Nature, 193, 293-294.
- Heyer K., Augustin, M., Protz, K., Herberger, K., Spehr, C. and Rustenbach, S. J. (2013). Effectiveness of Advanced versus Conventional Wound Dressings on Healing of Chronic Wounds - Systematic Review and Meta-Analysis. Dermatology, 226(2), 172-184.
- Jones, V., Grey, J. E. and Harding, K. G. (2006). Wound dressings. British Medical Journal, 332(7544), 777-780.
- Weinstein, M. L. (1998). Update on Wound Healing: A review of the Literature. Military Medicine, 163(9), 620-624
- Thomas, S. (1997). Assessment and management of wound exudate. Journal of Wound Care, 6(7), 327-330.
- Cohen, B. J. (2005) Chapter 13: The Blood. In Cohen, B. J. (Editor), The Human Body in Health and Disease. 10ed, 262-81.
- International Wound Infection Institute (IWII) (2016). Wound Infection in Clinical Practice - Principles of best practice. Wounds International. 1-32.
- Rodrigues, J., Mitta, N. (2011). Diabetic Foot and Gangrene. Gangrene - Current Concepts and Management Options, InTech 121-144
- EONS (2015). Recommendations for the Care of Patients with Malignant Fungating Wounds. European Oncology Nursing Society, 1-30.
- Junker, J. P. E., Kamel, R. A., Caterson, E. J. and Eriksson, E. (2013). Clinical Impact Upon Wound Healing and Inflammation in Moist, Wet, and Dry Environments. Advances in Wound Care, 2(7), 348-356.
- Ruben, B. (2014). Clearing the Air About Moist vs. Dry Wound Healing. Wound Source. Available at: www.woundsource.com
- Hurd T. (2012). Evaluating the costs and benefits of innovations in chronic wound care products and practices. Ostomy Wound Management, June, 1-15.
- Moffatt, C. J. (2002). Pain at wound dressing changes. EWMA Position Document, 1-18.
- Jones, V., Grey, J. E. and Harding, K. G. (2006). Wound dressings. British Medical Journal, 332(7544), 777-780.
- Ovington, L. G. (2001) Hanging Wet-to-Dry Dressings Out to Dry. Home Healthcare Nurse, 19(8) 477-484.
- Foster, L. and Moore, P. (1997). The application of cellulose fibre dressings in surgical wounds. Journal of Wound Care, 6(10), 469-473.
- Fleck, C. A. (2009). Why 'Wet to Dry'? Journal of the American College of Certified Wound Specialists, 1(4) 109-113
- Martin, M. (2013). Chapter 3: Physiology of Wound Healing. In Flanagan M. (Editor), Wound Healing and Skin Integrity. Principles and Practice (pp. 33-51). West Sussex: John Wiley & Sons, Ltd
- Dowsett et al. (2020). Closing the gap between the evidence and clinical practice – a consensus report on exudate management (11(3)) (def. exudate pooling)Snyder RJ Managing dead space: an overview. Podiatry Management. October 2005.
You may also be interested in…

HEAL e-learning
Learn about the benefits of moist wound healing with this EWMA-endorsed course.

Patient case
Learn how a venous leg ulcer was managed with a silicone foam dressing.

Triangle of Wound Assessment
Conduct a holistic and systematic wound assessment with our tool.