
Get full access with a free account
Benefits of the Coloplast® Professional Educational platform
- Get full access to all educational content, events and resources
- Track your progress
- Share content with your collegues
- Share supporting material with your patient
How to classify pressure injuries
In this section, you’ll learn:
How pressures injuries are classified
Thepressure injury classification system helps us describe the level of damage to the skin and tissue.1 This is an important first step in order to develop the right treatment plan for this type of injuries.
We classify pressure injuries based on the amount of tissue loss we can see. The deeper the wound, the more significant the tissue loss. The wound’s depth also determines what the body needs to do to heal the wound. For example, Stage 2 pressure injuries heal using a process called epithelialisation.1
On the other hand, in full-thickness pressure injuries (Stages 3 and 4), the body produces granulation tissue to heal.1 You will also see dead, or necrotic, tissue in full-thickness pressure injuries. The dead tissue may be slough and/or eschar.
What it looks like
How to recognise it
With Stage 1 pressure injuries, the skin is still intact. So there is no open wound. What you do find is an area of the skin that is reddened, and that remains red even after you apply pressure with your finger (non-blanchable erythema). Keep in mind that non-blanchable erythema may look different in patients with darker skin tones.2,3
What to keep in mind
It can be difficult to detect Stage 1 pressure injuries in patients with darker skin tones. Be sure conduct a full assessment of the surrounding skin as well.1
In Stage 2 pressure injuries, you have an open wound where you can see the dermis. The wound bed may be red or pink. However, Stage 2 injuries can also be blisters filled with clear fluid (serum), that are either intact or burst.
If your patient has darker skin, you should prioritise the following in your assessment:
- skin heat & tenderness
- changes in tissue consistency
- pain
You should do this for Stage 2-4 and unstageable pressure injuries.1
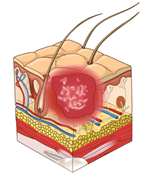
Stage 3: Full-thickness skin loss
In Stage 3 pressure injuries, you can see fat (adipose) in the wound. You might also see:
- granulation tissue
- rolled wound edges (epibole)
- slough/eschar (scabbing)
- undermining/tunnelling
However, you won’t be able to see muscle, tendons, ligaments or bone in a Stage 3 injury.2,3
Pressure injuries located on a part of the body with fatty tissue, such as the buttocks, may be deep but not reach the muscle or bone. You will still consider these types of injuries as Stage 3.1
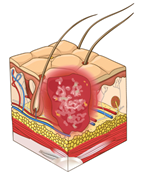
Stage 4: Full-thickness skin and tissue loss
In Stage 4 pressure injuries, fascia, muscle, tendon, ligament, cartilage or bone may be exposed or clearly visible in the wound.2,3
You can have shallow wounds that you would still classify as Stage 4. This could be if they are located on a part of the body with little fatty tissue, such as the bridge of the nose or behind the ear.1
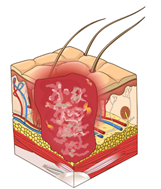
Unstageable: obscured full-thickness skin and tissue loss
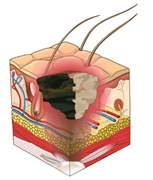
A pressure injury is unstageable when you cannot confirm how much tissue damage the wound has. In these cases, slough and/or eschar block the wound bed, so you cannot see how deep the wound is. However, if you remove the slough and/or eschar, you will find either a Stage 3 or Stage 4 pressure injury.2,3
Slough can be yellow, tan, grey, green or brown in colour. Eschar will either be tan, brown or black. Whether or not you should remove eschar to get a better look at the wound bed will depend on the eschar’s stability and where the pressure injury is located on the body. See our HEAL e-learning for more information here.2,3
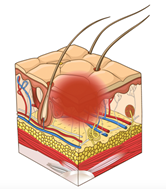
Deep tissue injury: Persistent, non-blanchable, deep red, maroon or purple discolouration
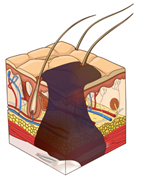
With deep tissue injuries, you may or may not see an open wound. If the skin is intact, it will have a deep red or purple colour. If there is an open wound, the wound bed will be dark. It might also have a blister filled with blood.3
If you can see dead tissue, fascia or muscle in the wound bed, then you should treat it as a full-thickness pressure injury (either Stage 3 or 4).3
References
- European Pressure Ulcer Advisory Panel. National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance. (2019) Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. Emily Haesler (Ed.) EPUAP/NPIAP/PPPIA.
- Edsberg, L. E., Black, J. M., Goldberg, M., McNichol, L., Moore, L. , Sieggreen, M. (2016). Revised National Pressure Injury Advisory Panel Pressure Injury Staging System. J Wound Ostomy Continence Nurs, 43(6), 1-13
- National Pressure Ulcer Advisory Panel (2016). National Pressure Ulcer Advisory Panel (NPUAP) announces a change in terminology from pressure ulcer to pressure injury and updates the stages of pressure injury. NPUAP: Washington. April 13, 1-3.
You may also be interested in…

HEAL e-learning
Learn how to assess and manage pressure injuries with this EWMA-endorsed course.
Managing the gap
Learn about the international consensus that was reached on managing the gap between the wound bed and the dressing.

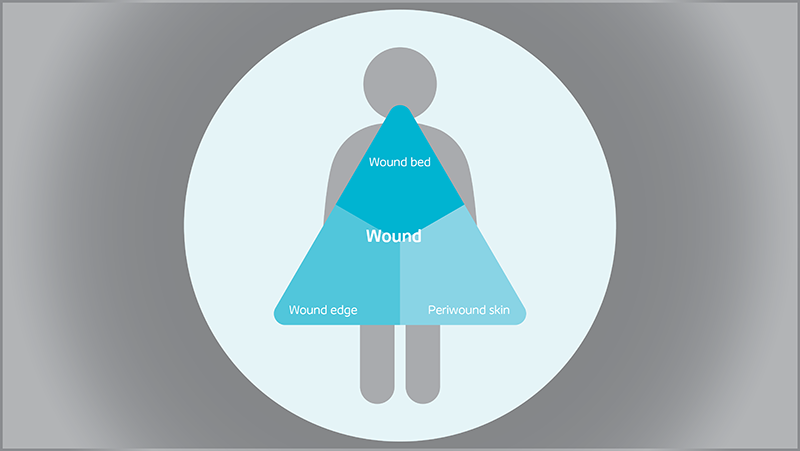
Triangle of Wound Assessment
Conduct a holistic and systematic wound assessment with our tool.