
Get full access with a free account
Benefits of the Coloplast® Professional Educational platform
- Get full access to all educational content, events and resources
- Track your progress
- Share content with your collegues
- Share supporting material with your patient
How to prevent pressure injuries
In this section, you’ll learn about:

Why a risk assessment is important?
Available risk assessment tools
There are three main assessment tools that can help you find out if your patient is at risk of developing a pressure injury:
- Braden Scale
- The Waterloo Scale
- The Norton Scale
For more information about these tools, take our HEAL Pressure Injury Prevention eLearning course.

How to conduct a skin assessment
Theskin is the body’s first line of defence.2 Changes to the skin can weaken the skin barrier. This makes the skin more vulnerable to pressure injuries – which is why assessing the skin is an important part of preventing pressure injuries.1
The goal of your skin assessment should be to assess, document and manage existing skin problems before a pressure injury develops. So you should look for signs of:
- dry skin
- moist skin
- paper-thin skin
- inflammation1
When you do your skin assessment, make sure to examine your patient from head to toe. Focus particularly on the skin overlying bony prominences, including the sacrum, ischial tuberosity, greater trochanters and the heels.1
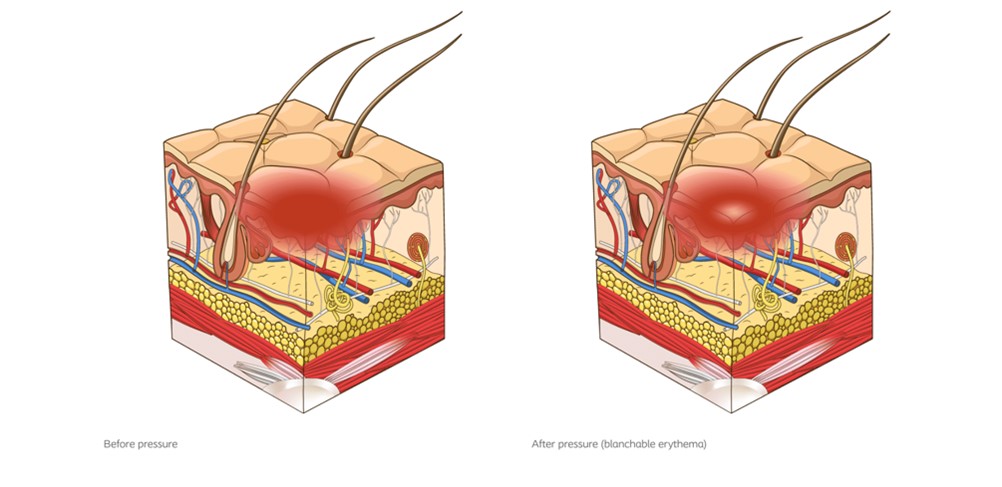
Blanchable erythema
With this type of erythema, the skin redness turns white when you apply pressure. It then turns red again, when you remove the pressure. It can mean that a pressure injury is about to develop.1
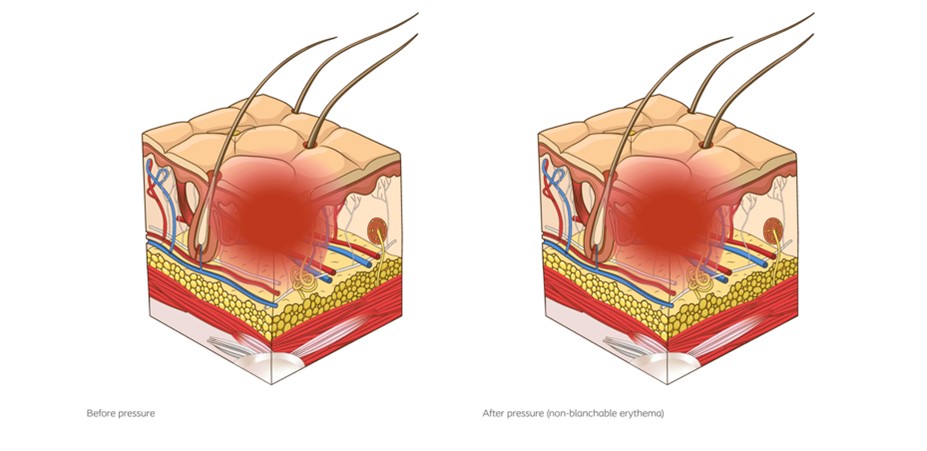
Non-blanchable erythema
With this type of erythema, the skin stays red, even after you apply pressure. If this happens, the capillary bed has been damaged. Non-blanchable erythema indicates a Stage 1 pressure injury.1
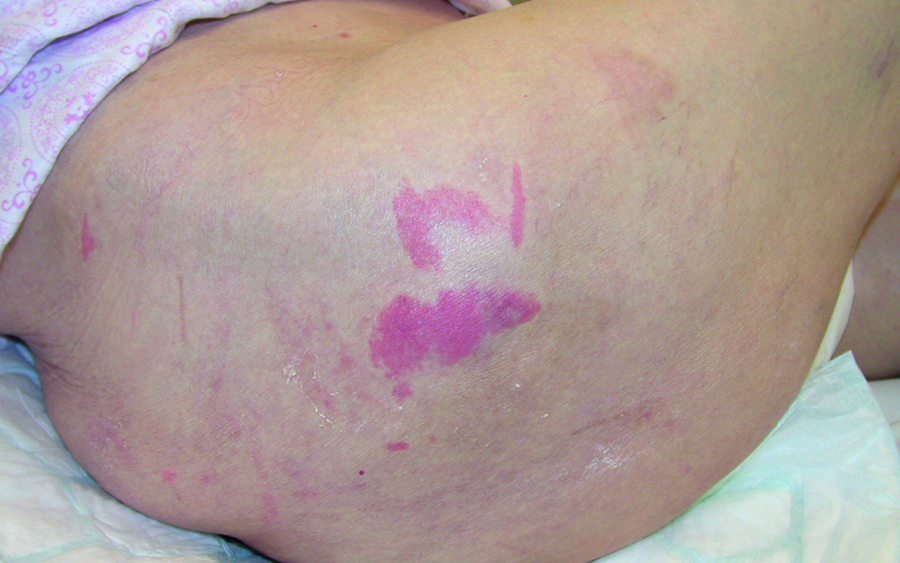
Assessing darkly pigmented skin
Studies suggest that it can be more difficult to see areas of erythema on darker skin tones. If your patient has darker skin, you should look for any areas of discolouration. If you find one, assess it closely. Look for:
- temperature changes
- oedema (excess fluid)
- changes in tissue consistency
- pain
How often should I conduct a skin assessment?
If you determine that your patient is at risk of developing a pressure injury, you should assess the skin and tissue:
- as soon as possible after they are admitted or transferred to the healthcare services;
- as a part of every risk assessment;
- periodically according to your patient’s risk level; and
- prior to discharge.
If you notice that your patient’s condition is getting worse, you should conduct an assessment more frequently. You can also conduct a brief skin assessment every time you reposition your patient.1
References
- European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (2019). Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guidelines. The International Guideline. Emily Haesler (Ed.). EPUAP/NPIAP/PPPIA.
- Baroni, A., Buommino, E., De Gregorio, V., Ruocco, E., Ruocco, V., Wolf, R. (2012). Structure and function of the epidermis related to barrier properties. Clinics in Dermatology, 30; 257-262.
You may also be interested in…

Patient case
Learn how a recurring pressure ulcer was managed with a silicone foam dressing.

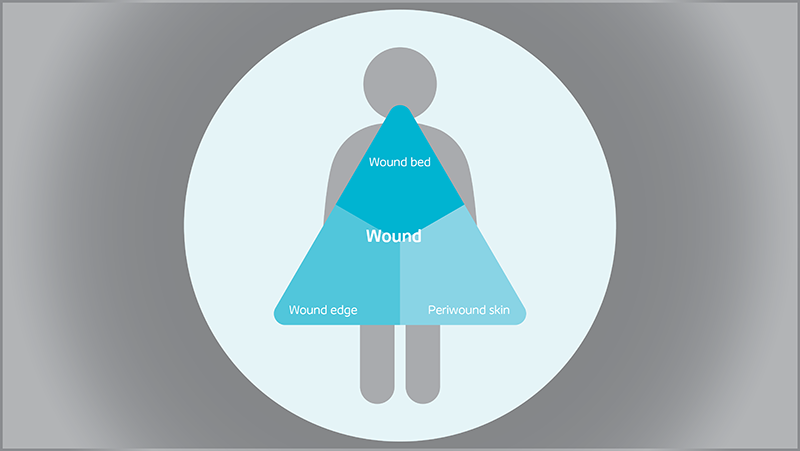
Triangle of Wound Assessment
Conduct a holistic and systematic wound assessment with our tool.