
Get full access with a free account
Benefits of the Coloplast® Professional Educational platform
- Get full access to all educational content, events and resources
- Track your progress
- Share content with your collegues
- Share supporting material with your patient
Pressure injuries: what are they and how do you prevent them?
In this section, you’ll learn about:
What is a pressure injury?
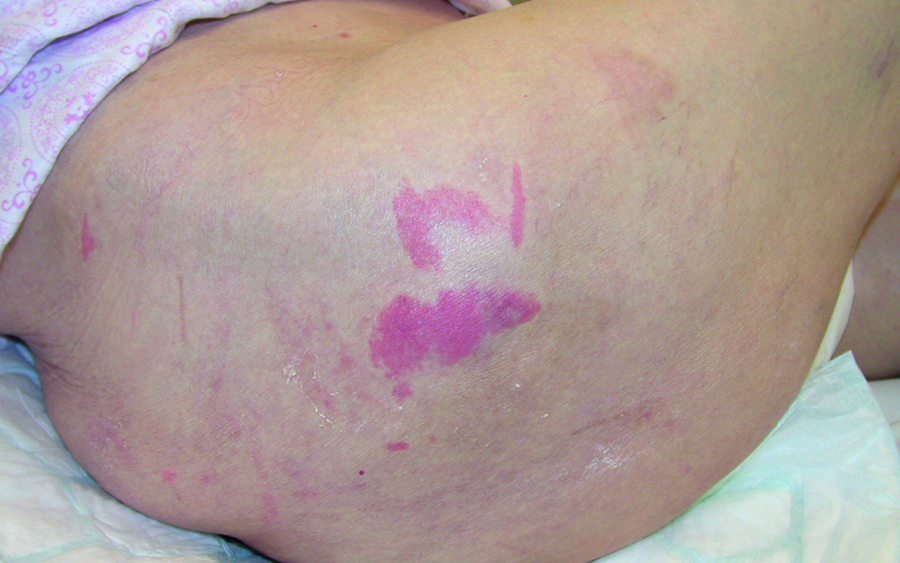
Pressureulcer, pressure sore, bedsore, pressure injury1– perhaps you’re familiar with one or all of these terms. They all refer to damage to the skin and/or underlying tissue that is caused by pressure, or the combination of pressure with shear.2
In a pressure injury, the skin can be intact or it can have an open wound. Pressure injuries are often quite painful for the patient.3
In the next section, we’ll take a closer look at where pressure injuries develop.
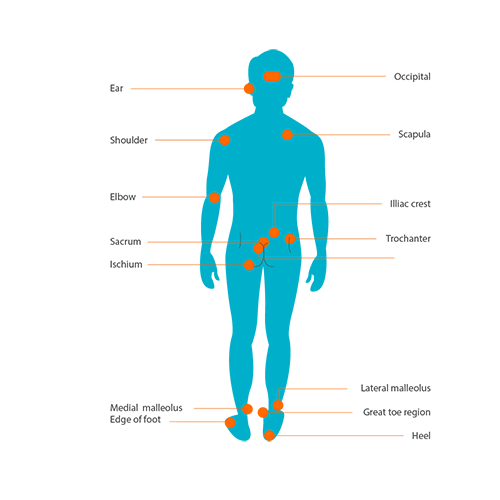
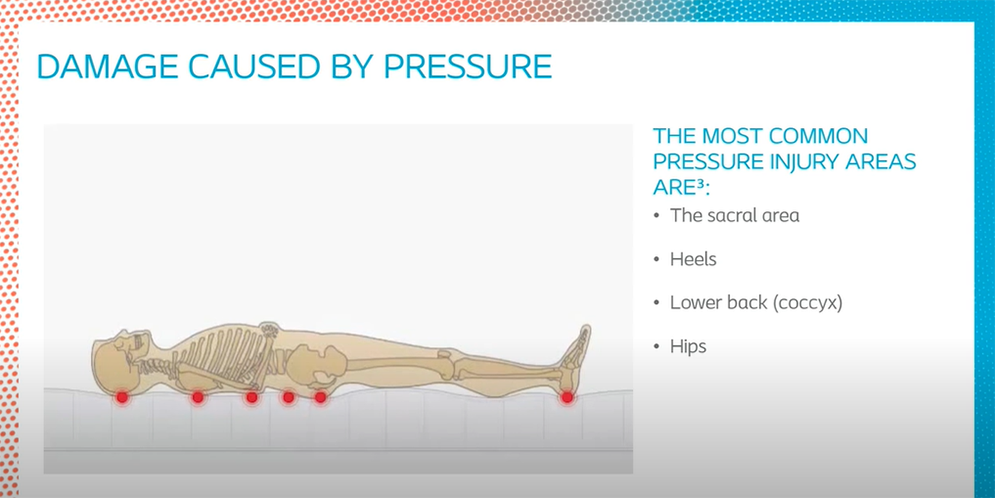
Most pressure injuries occur in the lower part of the body.4
Surveys show that the sacrum is the most common pressure injury site among patients in acute care facilities. The second most common site is the heel.4
However, pressure injuries can also occur on the elbows, ears, back of the head and the shoulder blades. These areas are often overlooked.4
How does a pressure injury form?
Pressure injuries form in two ways:
- when the skin is exposed to pressure that is either intense and/or prolonged; or
- when the skin is exposed to pressure combined with shear.5
How pressure can damage the skin
When pressure is applied to the skin, it distorts the skin and underlying tissues.6 This is particularly the case if the pressure is applied over a bony prominence. Pressure narrows the space between the bony prominence and the skin surface. This compresses the capillaries, meaning blood cannot flow properly to this area of the body. If the pressure continues, the soft tissue will die. This leads to skin damage – and ultimately, a pressure injury.4
To see how pressure can damage the skin, watch this video.

How pressure combined with shear can damage the skin
Now let’s look at the second way pressure injuries can develop.
Shear often occurs when a bedbound patient needs to change position. If the patient lies flat on their back, and the head of the bed is raised, the patient slides down the mattress. This sliding movement, combined with the pressure of the mattress, causes shear.
The pressure from the mattress compresses the blood capillaries. And shear (the sliding motion) distorts them. This increases the risk of a pressure injury developing.6
Watch this video to see how shear can damage the skin.
Did you know?
Lying with the backrest at an angle of 45° creates a high combination of shear stress and pressure on a patient’s buttocks and sacral area.6 This is where the most severe pressure injuries occur.2
Who are at risk of getting pressure injuries?
Whilethere are a wide range of factors that can contribute to pressure injuries,7 we will focus on two major risk factors: lack of mobility and skin moisture.
Lack of mobility
Changing position is an important way of relieving pressure areas. If patients cannot move, they cannot relieve the pressure. This can lead to pressure damage to the skin and underlying tissue.4,6, 8
This risk increases when:
- patients are too weak to turn or reposition themselves;
- they feel pain or discomfort when they move; or
- they don’t know they need to move about in bed.9
Learn how to reposition immobile patients here.

Skin moisture
The integrity of the skin plays an important role in preventing injuries. If a patient’s skin is too moist, or if it’s exposed to harmful moisture, this can weaken the skin. This could be moisture from:
- sweat;
- urine and/or stool; or
- wound exudate (or fluid).8
For example, when moisture from urine and/or stool gets on the skin, this can cause the skin to break down.8 This makes it more vulnerable to pressure-related injury.10, 11
Read more about how you can prevent pressure injuries in patients with incontinence here.
Assessing the skin is an important part of any pressure injury risk assessment.2 You can read more about how to protect the skin here.
Did you know?
Other factors can make the skin and soft tissue more vulnerable to pressure injuries. These factors include:
- the soft tissue’s condition;
- microclimate;
- nutrition;
- blood flow (perfusion); and
- co-morbidities.
References
- Advances in Skin and Wound Care (2004). By the numbers: Braden score interventions. Apr; 17(3): 150
- European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance (2019). Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guidelines. The International Guideline. Emily Haesler (Ed.). EPUAP/NPIAP/PPPIA.
- Ayello, E. A., Baranoski, S., Cuddigan, J. E. Harris, W. S. (2016). Chapter 13: Pressure Ulcers. In Baranoski, S., Ayello, E. A. (Editor), Wound Care Essentials – Practice Principles. 4th edition. Wolters Kluwer: Philadelphia.
- Agrawal, K., Chauhan, N. (2012). Pressure ulcers: Back to the basics. Indian Journal of Plastic Surgery. May-Aug; 45(2): 244–254.
- Edsberg, L. E., Black, J. M., Goldberg, M., McNichol, L., Moore, L. , Sieggreen, M. (2016). Revised National Pressure Injury Advisory Panel Pressure Injury Staging System. J Wound Ostomy Continence Nurs, 43(6), 1-13
- Wounds International. (2010). International review. Pressure ulcer prevention: pressure, shear, friction and microclimate in context. A consensus document. London: MEP Ltd.
- You can learn more about the other risk factors that can lead to pressure injuries in the Prevention and Treatment of Pressure Ulcers/Injuries Clinical Practice Guidelines – The International Guidelines 2019.
- Langemo, D. K. (2016). Chapter 23: Palliative Wound Care. In Baranoski, S., Ayello, E. A. (Editor), Wound Care Essentials – Practice Principles. 4th edition. Wolters Kluwer: Philadelphia.
- National Pressure Ulcer Advisory Panel (2016). National Pressure Ulcer Advisory Panel (NPUAP) announces a change in terminology from pressure ulcer to pressure injury and updates the stages of pressure injury. NPUAP: Washington. April 13, 1-3.
- Beeckman, D., Schoonhoven, L., Fletcher, J., Furtado, K., Gunningberg, L., Heyman, H., Lindholm, C., Paquay, L., Verdú, J. and Defloor, T. (2007). EPUAP classification system for pressure ulcers: European reliability study. Journal of Advanced Nursing, 60(6), 682-691.
- Brienza, D. M., Zulkowski, K., Sprigle, S., Geyer, M. J. (2016). Chapter 11: Pressure Redistribution: Seating, Positioning, and Support Surfaces. In Baranoski, S., Ayello, E. A. (Editor), Wound Care Essentials – Practice Principles. 4th edition. Wolters Kluwer: Philadelphia.
You may also be interested in…

Patient case
Learn how a pressure ulcer on the right lower limb was managed with a silicone foam dressing.

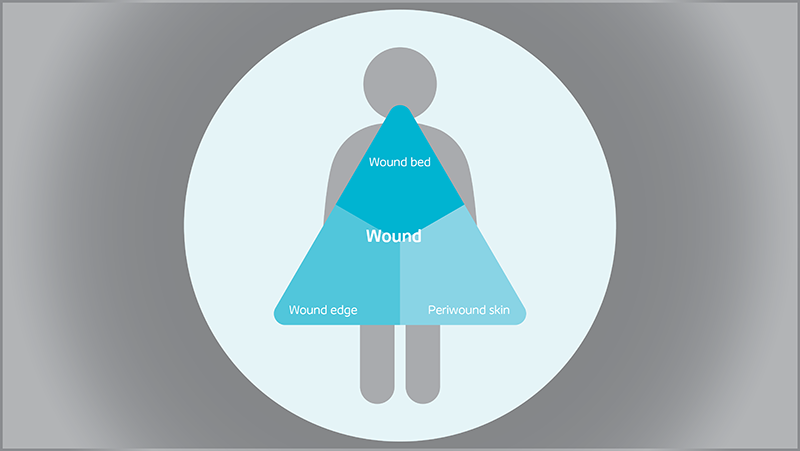
Triangle of Wound Assessment
Conduct a holistic and systematic wound assessment with our tool.